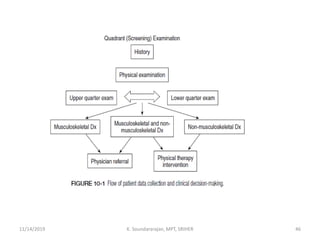
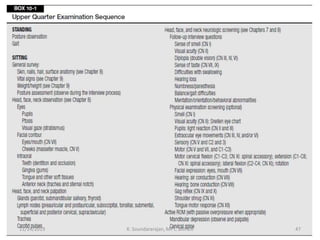
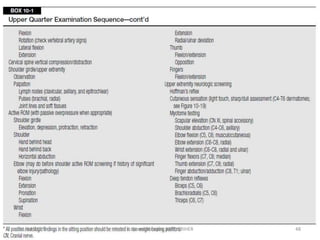
This document discusses musculoskeletal examination techniques used by physical therapists. It covers screening examinations to identify red flags and impairments, as well as detailed examinations of mobility, muscle performance, joints, gait, and pain. Techniques include observation, palpation of bones, muscles, and joints, range of motion and strength testing, and functional assessments. The goal is to comprehensively evaluate patients and guide diagnosis, treatment planning, and outcomes.