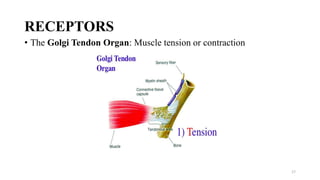
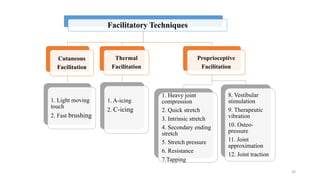
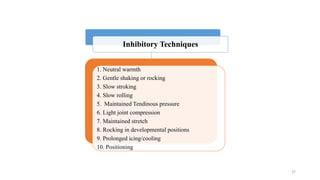
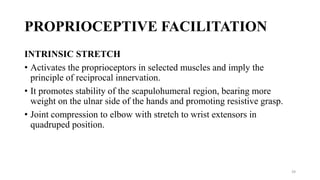
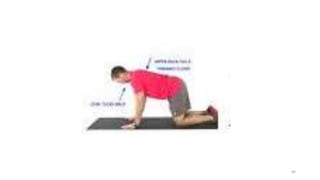
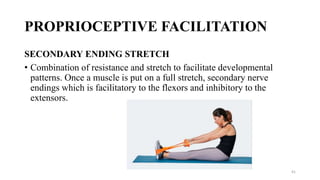
The document discusses various facilitation and inhibition techniques used in physical therapy, outlining the theoretical basis, principles, receptors involved, differences between the techniques, guidelines for application, and clinical implications. It provides detailed descriptions of numerous proprioceptive and cutaneous facilitation techniques including quick stretch, tapping, joint compression, as well as inhibitory techniques like maintained stretch and cooling. The techniques aim to normalize muscle tone and facilitate or inhibit motor responses depending on a patient's needs.