Download free for 30 days
Sign in
Upload
Language (EN)
Support
Business
Mobile
Social Media
Marketing
Technology
Art & Photos
Career
Design
Education
Presentations & Public Speaking
Government & Nonprofit
Healthcare
Internet
Law
Leadership & Management
Automotive
Engineering
Software
Recruiting & HR
Retail
Sales
Services
Science
Small Business & Entrepreneurship
Food
Environment
Economy & Finance
Data & Analytics
Investor Relations
Sports
Spiritual
News & Politics
Travel
Self Improvement
Real Estate
Entertainment & Humor
Health & Medicine
Devices & Hardware
Lifestyle
Change Language
Language
English
Español
Português
Français
Deutsche
Cancel
Save
Submit search
EN
Uploaded by
shadiac
27,097 views
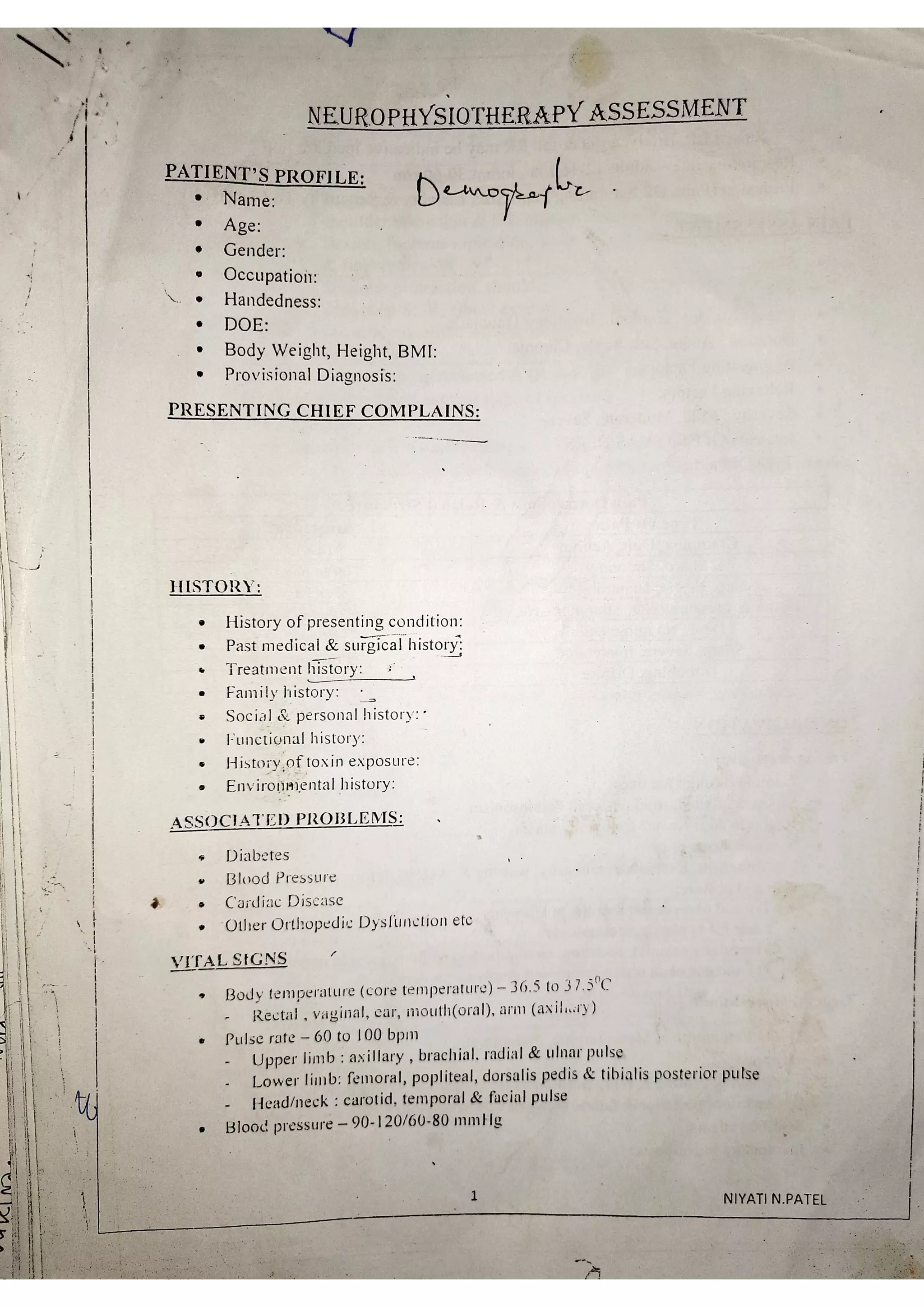
NEURO PHYSIOTHERAPY ASSESSMENT
NEURO PHYSIOTHERAPY ASSESSMENT
Education
◦
Read more
7
Save
Share
Embed
Embed presentation
Download
Downloaded 38 times
1
/ 23
2
/ 23
Most read
3
/ 23
Most read
4
/ 23
Most read
5
/ 23
6
/ 23
7
/ 23
8
/ 23
9
/ 23
10
/ 23
11
/ 23
12
/ 23
13
/ 23
14
/ 23
15
/ 23
16
/ 23
17
/ 23
18
/ 23
19
/ 23
20
/ 23
21
/ 23
22
/ 23
23
/ 23
More Related Content
PDF
stroke assessment format
by
shadiac
PDF
Kaplan National Physical Therapy Exam by Bethany Chapman Mary Fratianni
by
Shahsad Aboobacker
PPTX
Paediatric Assessment in Physiotherapy.pptx
by
HanineHassan2
PPTX
BOBATH_THERAPY_HIMANIKAUSHIK.pptx
by
Himani Kaushik
PPTX
physiotherapy in MND.pptx
by
ibtesaam huma
PDF
Proprioceptive Neuromuscular Facilitation (PNF)
by
Ashik Dhakal
PPTX
Brunnstrom Approach
by
Himani Kaushik
PPTX
Physiotherapy management of Multiple sclerosis
by
Keerthi Priya
stroke assessment format
by
shadiac
Kaplan National Physical Therapy Exam by Bethany Chapman Mary Fratianni
by
Shahsad Aboobacker
Paediatric Assessment in Physiotherapy.pptx
by
HanineHassan2
BOBATH_THERAPY_HIMANIKAUSHIK.pptx
by
Himani Kaushik
physiotherapy in MND.pptx
by
ibtesaam huma
Proprioceptive Neuromuscular Facilitation (PNF)
by
Ashik Dhakal
Brunnstrom Approach
by
Himani Kaushik
Physiotherapy management of Multiple sclerosis
by
Keerthi Priya
What's hot
PPTX
vojta therapy
by
Dr. PETETI SAIRAM
PPT
Iliotibial Band Syndrome (Itbs)
by
colinmasterson
PPTX
Tendon tranfer
by
Prasanthmuddada
PPTX
Cardio PT assessment
by
Dr Samir Jadav
PPT
Hydrocephalus
by
Dr. Rima Jani (PT)
PPTX
Leprosy & its pt management
by
SwetaUpadhyay5
PDF
Disability evaluation
by
Radhika Chintamani
PPTX
Neurological Gait Rehabilitation
by
Dr. Rima Jani (PT)
PPTX
Spasticity management
by
JWANIKA VANSIYA
PPTX
Voluntary Control and Assessment Physiotherapy Perspective.pptx
by
Susan Jose
PPTX
Physiotherapy for CONGENITAL TALIPES EQUINOVARUS
by
Sreeraj S R
PDF
SENSORY ASSESSMENT.pdf
by
Suvarna JaipurkarGanvir
PPT
Myofacial Release Therapy(MFR).
by
Dr.Debanjan Mondal(PT)
PPTX
Rotator cuff injuries
by
pratigya deuja
PPTX
COORDINATION.pptx
by
Sanam227891
PPT
Pnf respiratory
by
Apatel99094
PPTX
Supraspinatus tendinitis 30may2013
by
Rahila Najihah
PPT
Bobath therapy.ppt
by
Dr. Jasjyot
PPTX
SI JOINT DYSFUNCTION.pptx
by
kajal sansoya
PPTX
Frozen Shoulder Physiotherapy Management
by
Vishal Deep
vojta therapy
by
Dr. PETETI SAIRAM
Iliotibial Band Syndrome (Itbs)
by
colinmasterson
Tendon tranfer
by
Prasanthmuddada
Cardio PT assessment
by
Dr Samir Jadav
Hydrocephalus
by
Dr. Rima Jani (PT)
Leprosy & its pt management
by
SwetaUpadhyay5
Disability evaluation
by
Radhika Chintamani
Neurological Gait Rehabilitation
by
Dr. Rima Jani (PT)
Spasticity management
by
JWANIKA VANSIYA
Voluntary Control and Assessment Physiotherapy Perspective.pptx
by
Susan Jose
Physiotherapy for CONGENITAL TALIPES EQUINOVARUS
by
Sreeraj S R
SENSORY ASSESSMENT.pdf
by
Suvarna JaipurkarGanvir
Myofacial Release Therapy(MFR).
by
Dr.Debanjan Mondal(PT)
Rotator cuff injuries
by
pratigya deuja
COORDINATION.pptx
by
Sanam227891
Pnf respiratory
by
Apatel99094
Supraspinatus tendinitis 30may2013
by
Rahila Najihah
Bobath therapy.ppt
by
Dr. Jasjyot
SI JOINT DYSFUNCTION.pptx
by
kajal sansoya
Frozen Shoulder Physiotherapy Management
by
Vishal Deep
Recently uploaded
PPTX
CHAPTER NO. 05 BIOLOGICAL SOURCE,CHEMICAL CONSTITUENTS AND THERAPEUTIC EFFICA...
by
Ganu Gavade
PDF
Gaming Quiz 2025- 27th October 2025, Quiz Club NITW
by
Quiz Club NITW
PPTX
OCCULTISM IN JEHOVAH'S WITNESSES' ARTWORK
by
Daniel Barnea
PDF
Fever & Fragment Uncovering the Plague in The Waste Land
by
Nidhi Pandya
PPTX
L5 DRG Pulsed Radiofrequency ablation.pptx
by
Sandeep Margan
PPTX
Cultivation Practice of Potato in Nepal.pptx
by
UmeshTimilsina1
PDF
Life-Processes-in-Animals PPT/7TH CLASS NEW NCERT /CURIOSITY SCIENCE /BY K SA...
by
Sandeep Swamy
PPT
Blood Grouping.ppt - Hematology -Physiology
by
kishorkumar396
PPT
Clotting time - Practical - Hematology Physiology
by
kishorkumar396
PDF
Teaching and Learning (BD1TL) - B.Ed TNTEU
by
Dr Raja Mohammed T
PPTX
Introduction to Mendelian inheritance.pptx
by
pramodphirke1
PPTX
Cultivation practice of Cucumber, Pumpkin and summer squash in Nepal.pptx
by
UmeshTimilsina1
PDF
How to Report Cyber Fraud in India: Your Digital First Aid Kit (2025 Guide)
by
Sanjay Rathod
PDF
Digital_Empathy_Toolkit_Netiquette_and_Responsible_Communication
by
Nidhi Pandya
PPTX
Salesforce Spring 26` Release Key Features.pptx
by
MehediHasan939830
PDF
India Cybercrime Threats & Response 2025: Digital Arrests, 1930 Helpline & Ze...
by
Sanjay Rathod
PPTX
YSPH VMOC Special Report - Measles - The Americas 12-28 2025 .pptx
by
Yale School of Public Health - The Virtual Medical Operations Center (VMOC)
PPTX
Cultivation practice of Root vegetables.pptx
by
UmeshTimilsina1
PDF
The Industrialisation of Deception: An Analysis of the 2024 Cybercrime Landscape
by
krutivyas2005
PDF
Renewable Energy Resources Unit 2 Easy notes (EduShine Classes).pdf
by
aaquib913
CHAPTER NO. 05 BIOLOGICAL SOURCE,CHEMICAL CONSTITUENTS AND THERAPEUTIC EFFICA...
by
Ganu Gavade
Gaming Quiz 2025- 27th October 2025, Quiz Club NITW
by
Quiz Club NITW
OCCULTISM IN JEHOVAH'S WITNESSES' ARTWORK
by
Daniel Barnea
Fever & Fragment Uncovering the Plague in The Waste Land
by
Nidhi Pandya
L5 DRG Pulsed Radiofrequency ablation.pptx
by
Sandeep Margan
Cultivation Practice of Potato in Nepal.pptx
by
UmeshTimilsina1
Life-Processes-in-Animals PPT/7TH CLASS NEW NCERT /CURIOSITY SCIENCE /BY K SA...
by
Sandeep Swamy
Blood Grouping.ppt - Hematology -Physiology
by
kishorkumar396
Clotting time - Practical - Hematology Physiology
by
kishorkumar396
Teaching and Learning (BD1TL) - B.Ed TNTEU
by
Dr Raja Mohammed T
Introduction to Mendelian inheritance.pptx
by
pramodphirke1
Cultivation practice of Cucumber, Pumpkin and summer squash in Nepal.pptx
by
UmeshTimilsina1
How to Report Cyber Fraud in India: Your Digital First Aid Kit (2025 Guide)
by
Sanjay Rathod
Digital_Empathy_Toolkit_Netiquette_and_Responsible_Communication
by
Nidhi Pandya
Salesforce Spring 26` Release Key Features.pptx
by
MehediHasan939830
India Cybercrime Threats & Response 2025: Digital Arrests, 1930 Helpline & Ze...
by
Sanjay Rathod
YSPH VMOC Special Report - Measles - The Americas 12-28 2025 .pptx
by
Yale School of Public Health - The Virtual Medical Operations Center (VMOC)
Cultivation practice of Root vegetables.pptx
by
UmeshTimilsina1
The Industrialisation of Deception: An Analysis of the 2024 Cybercrime Landscape
by
krutivyas2005
Renewable Energy Resources Unit 2 Easy notes (EduShine Classes).pdf
by
aaquib913
Download