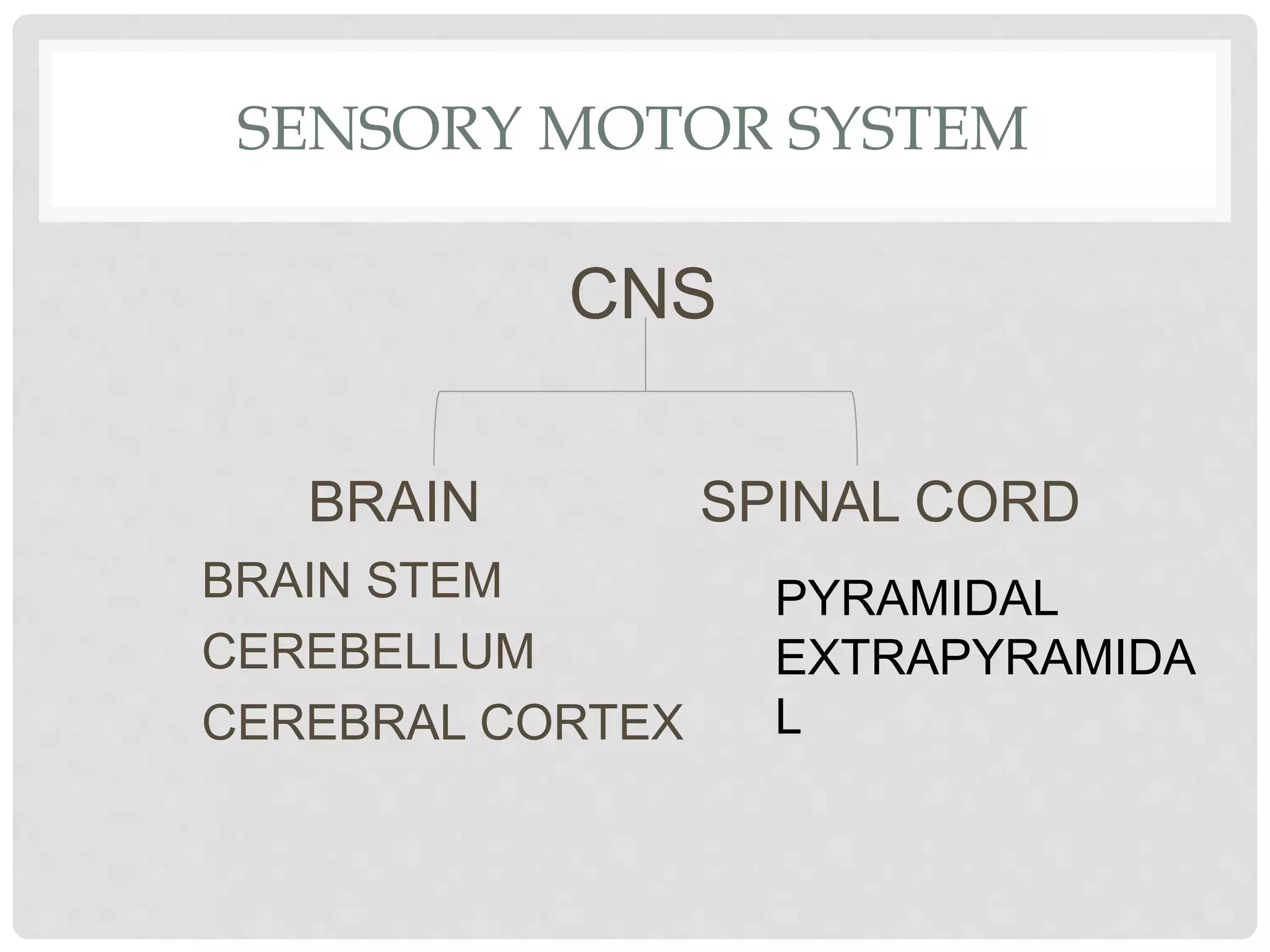
This document discusses Rood's sensory motor approach for gaining motor control in patients. It describes the levels of motor control from reflex mobility to skilled movement. Sensory inputs like light touch, vibration and vestibular stimulation can facilitate movement while rocking inhibits it. Proprioceptive techniques like stretching and resistance activate muscles. The document also outlines Rood's principles of using activity to demand purposeful response and practicing sensory motor responses for motor learning.