

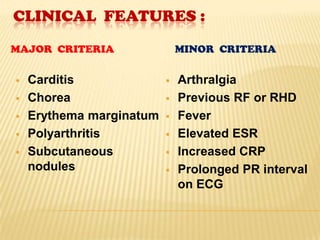











Rheumatic fever is an inflammatory disease that occurs after a streptococcal throat infection. It affects the heart, joints, skin, and brain. While rates have declined due to improved living standards, rheumatic heart disease remains an issue in India, with reported incidence varying from 0.12-11 cases per 1000 people. Rheumatic fever is diagnosed using modified Jones criteria of either two major symptoms or one major and two minor symptoms. Treatment focuses on bed rest, antibiotics to treat strep infections, aspirin, and managing symptoms like chorea. The goals are to eliminate strep bacteria, prevent permanent heart damage, palliate symptoms, and prevent recurrence.

















































































