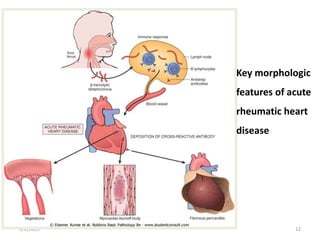
Rheumatic fever is an inflammatory disease that can occur after a streptococcal throat infection. It involves the heart, joints, skin and connective tissue. The presentation includes fever, arthritis and heart complications like pancarditis. Diagnosis is based on clinical criteria after excluding other conditions. Prevention relies on prompt antibiotic treatment of streptococcal infections. For those with a history of rheumatic fever, long-term antibiotic prophylaxis is needed to prevent recurrences that can further damage the heart.