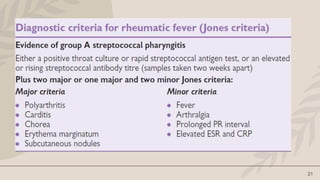
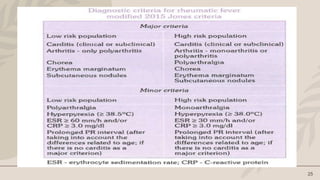
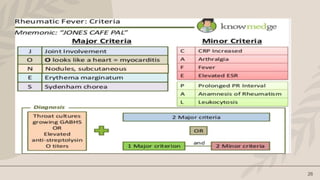
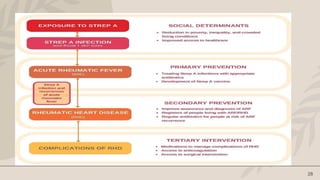
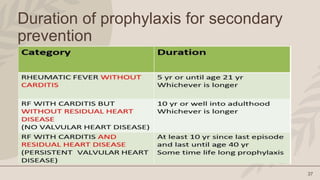
Rheumatic heart disease is caused by a prior streptococcal throat infection and leads to damage of the heart valves over time. It is a major public health problem globally and in India, where there are approximately 1 million cases. The Jai Vigyan Mission Mode project in India conducted epidemiological studies of streptococcal infections and established registries for rheumatic fever and rheumatic heart disease. Rheumatic heart disease is diagnosed using revised Jones criteria and treated with long-term antibiotic prophylaxis to prevent recurrent streptococcal infections and further valve damage. Prevention through proper treatment of streptococcal infections is critical to reducing the burden of rheumatic heart disease worldwide.




































![Acute Rheumatic Fever – An Update[6704].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuterheumaticfeveranupdate6704-250603154932-9410381d-thumbnail.jpg?width=640&height=640&fit=bounds)






































