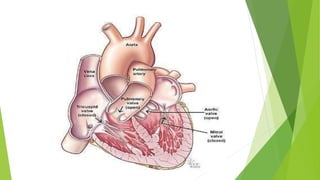
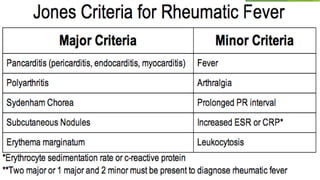
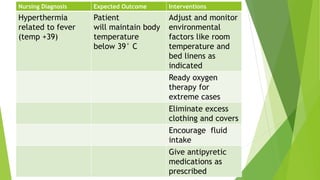
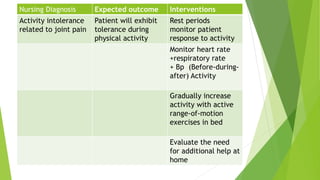
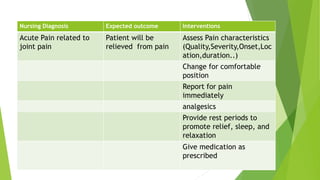
Rheumatic heart disease is caused by rheumatic fever, which occurs as a complication of untreated strep throat. It leads to damage of the heart valves. Symptoms include fever, joint pain, and heart murmurs. Treatment involves antibiotics to eliminate strep bacteria and anti-inflammatory drugs. Nursing care focuses on monitoring for symptoms, managing pain and fever, restricting activity, and teaching about prevention and treatment adherence. Complications can include heart failure, arrhythmias, and valve damage if not properly treated.