This document provides an overview of retinoblastoma, including:
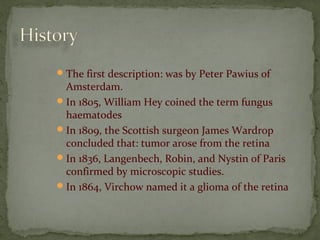
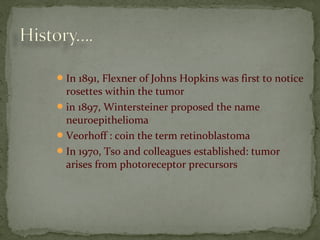
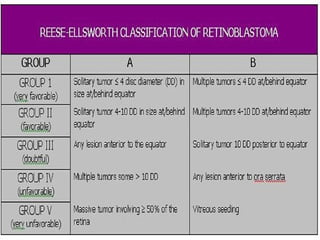
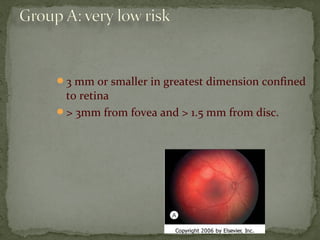
1. A brief history of retinoblastoma classification and descriptions.
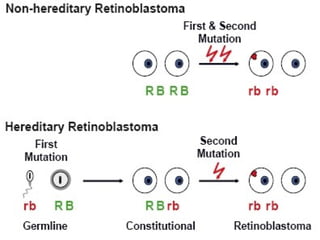
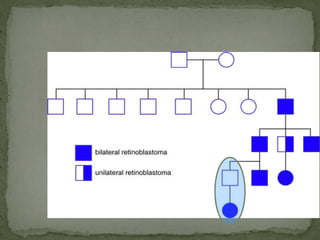
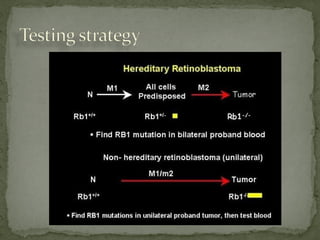
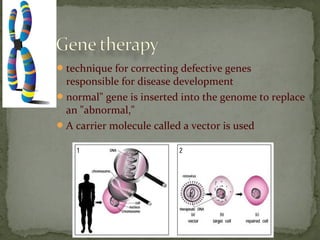
2. Details on the genetics and pathogenesis of retinoblastoma, including the two-hit hypothesis.
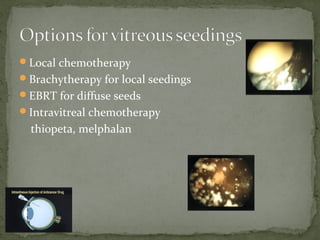
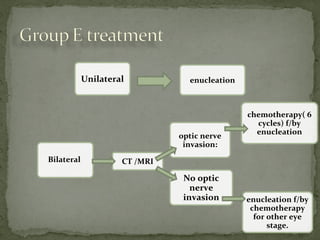
3. Presenting features, diagnostic testing, classification systems, and treatment options for retinoblastoma such as chemotherapy, radiation therapy, cryotherapy, and enucleation.

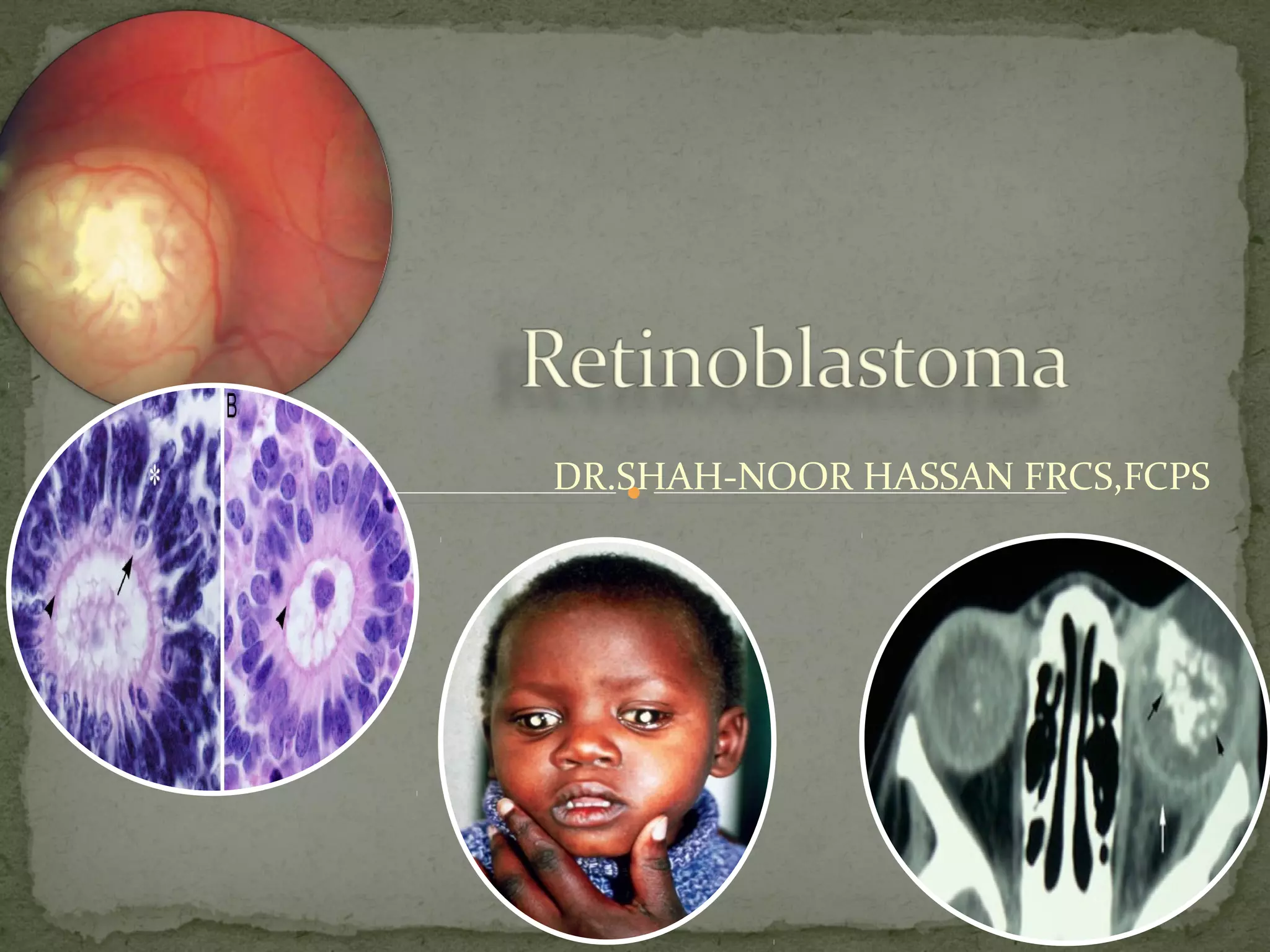
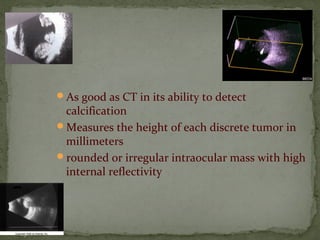
![Retinoblastoma is a rare childhood cancer.
third most common cancer overall affecting
children
3% of all cancers in children younger than 15
years of age
National Cancer Institute [NCI], 2007
most common intraocular malignant neoplasm
in children (Castillo and Kaufman, 2003).](https://image.slidesharecdn.com/retinoblastomapre-180318103316/85/Retinoblastoma-Rb-4-320.jpg)





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






