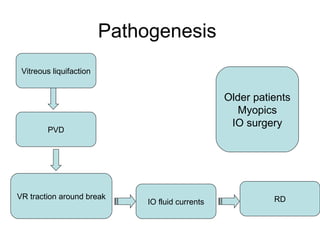
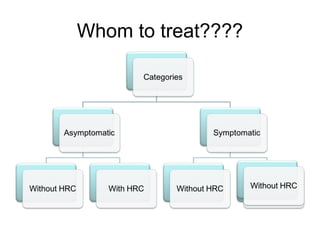
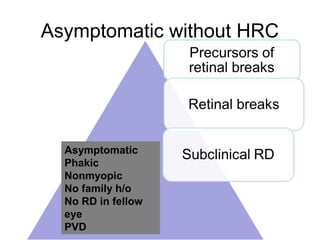
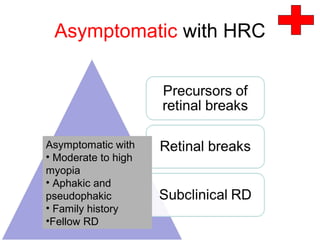
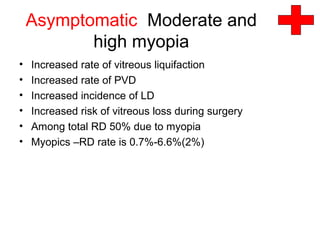
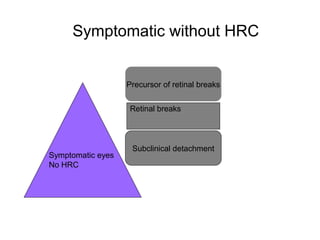
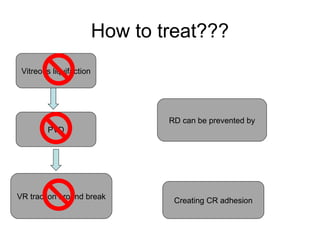
The document discusses the pathogenesis and prophylaxis of retinal detachment (RD), highlighting its significant impact on vision and potential blindness, specifically in older, myopic patients. It outlines various risk factors, treatment options, and the conditions under which prophylactic treatments can be applied, emphasizing the importance of categorizing patients based on their predisposition to RD. Despite the availability of surgical intervention, the success rate remains moderate, with many patients experiencing less than optimal vision outcomes post-surgery.













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






