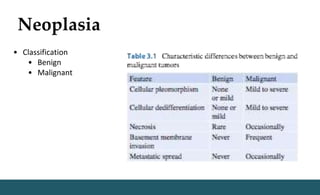
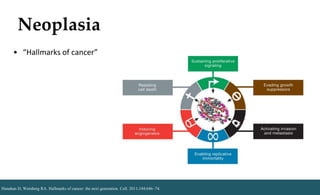
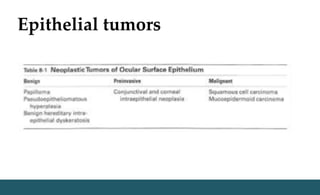
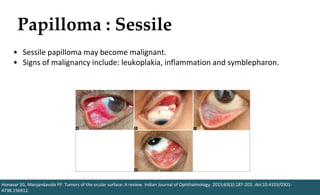
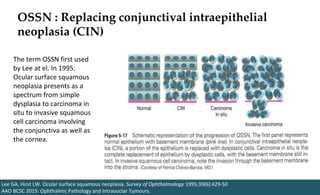
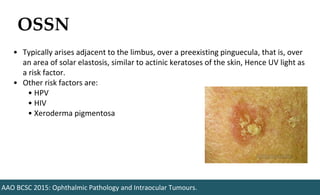
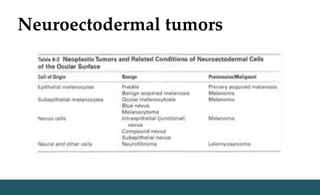
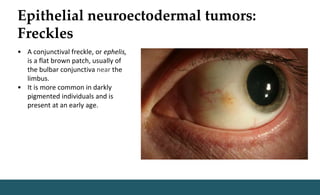
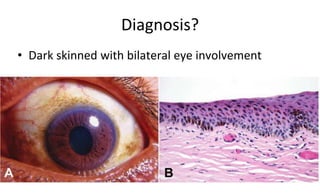
Benign epithelial tumors of the ocular surface include papillomas, which are caused by HPV infection and can be either pedunculated or sessile. Sessile papillomas have a risk of malignant transformation. Malignant epithelial tumors include ocular surface squamous neoplasia (OSSN), which presents as dysplasia or carcinoma in situ and can invade the cornea or globe if not treated with surgical excision or topical chemotherapy. Neuroectodermal tumors of the ocular surface include freckles, benign acquired melanosis (BAM), and primary acquired melanosis (PAM), which has a risk of progressing to conjunctival melanoma. Close monitoring is important to detect malignant transformation



![OSSN: Epidemiology
Radhakrishnan A. Ocular Surface Squamous Neoplasia [OSSN] - A Brief Review. KSOS 2011; XXIII(4)
➢ Third most common ocular tumor after melanoma,
lymphoma.
➢ Australia: OSSN accounts for 10% of all pterygia excised.](https://image.slidesharecdn.com/ocularsurfaceneoplasiaforslideshare-190927065240/85/Ocular-surface-neoplasia-32-320.jpg)
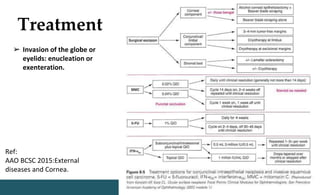
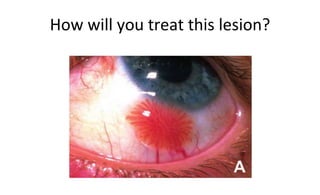
![Treatment
Radhakrishnan A. Ocular Surface Squamous Neoplasia [OSSN] - A Brief Review. KSOS 2011; XXIII(4)
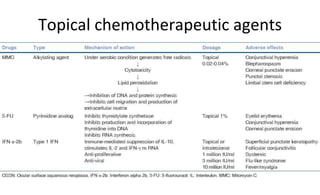
• If topical chemotherapeutic agents are used:
• Punctal occlusion
• Avoid in pregnancy
• Side-effects;
• Ocular surface toxicity
• Epithelial defects
• Cataract
• Punctal stenosis](https://image.slidesharecdn.com/ocularsurfaceneoplasiaforslideshare-190927065240/85/Ocular-surface-neoplasia-37-320.jpg)











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














