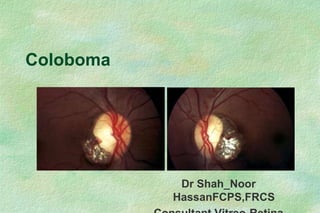
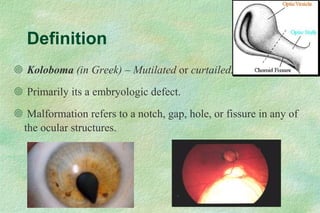
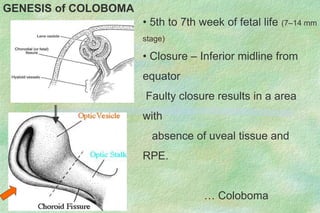
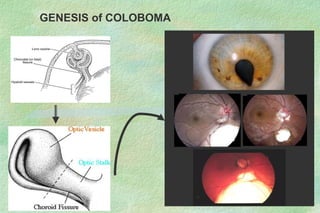
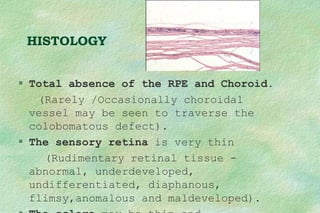
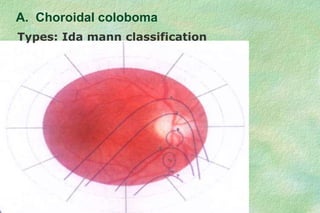
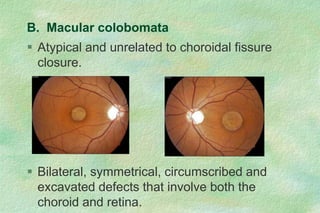
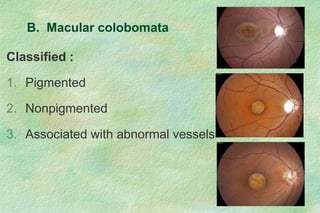
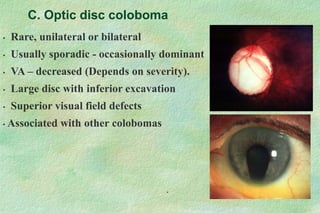
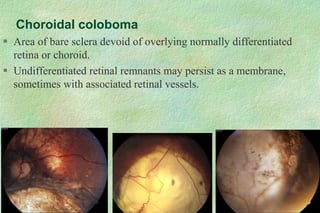
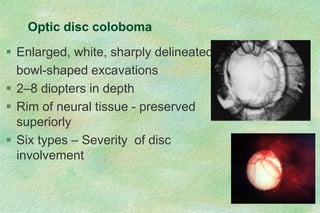
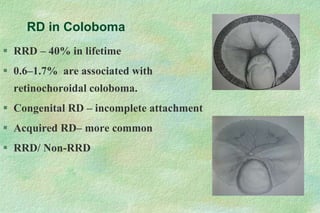
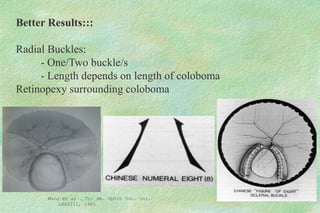
Coloboma is an embryologic ocular defect characterized by a gap or hole in ocular structures, with an incidence of 0.14% and typically bilateral occurrences. The classification of colobomas includes types based on location and completeness, with associated clinical features like visual field defects and retinal detachments being common complications. Treatment options vary depending on the severity and location of the defect, encompassing surgical interventions and management of associated conditions such as cataracts and retinal detachments.