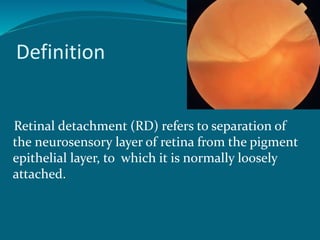
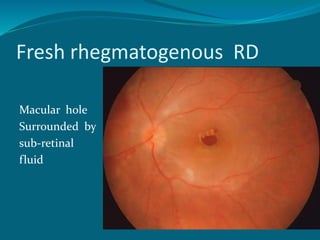
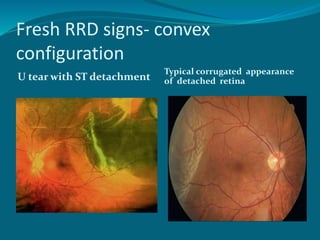
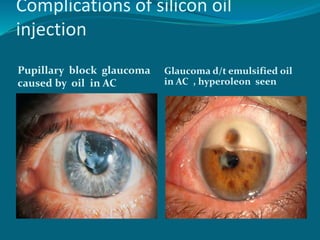
This document provides an overview of retinal detachment, including its definition, types, signs, symptoms, and management. It discusses the four main types - rhegmatogenous, tractional, exudative, and combined tractional-rhegmatogenous. Rhegmatogenous retinal detachment is the most common type, characterized by a retinal break allowing fluid accumulation under the retina. The document describes treatments like scleral buckling, pneumatic retinopexy, and vitrectomy. It also reviews complications of various surgical procedures and use of tamponading agents like gases and silicone oil.