Retinal detachment
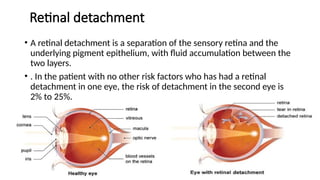
• Aretinal detachment is a separation of the sensory retina and the
underlying pigment epithelium, with fluid accumulation between the
two layers.
• . In the patient with no other risk factors who has had a retinal
detachment in one eye, the risk of detachment in the second eye is
2% to 25%.
4.
Predisposing factors
Age :Thecondition is most common in 40-60 years. However, age is no
bar.
• Sex :More common in males (M:F-3:2).
• myopia
• previous intraocular surgery such as aphakia or pseudophakia,
• a family history of retinal detachment
• Trauma and inflammation.
• Retinal necrosis with the formation of retinal breaks can occur in the
ARN syndrome and in cytomegalovirus retinitis.
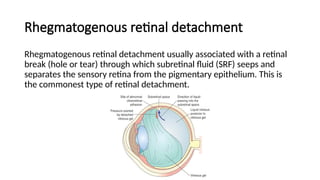
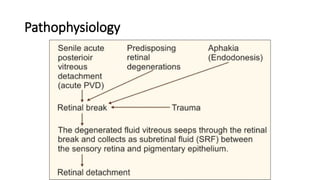
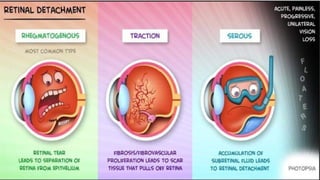
Rhegmatogenous retinal detachment
Rhegmatogenousretinal detachment usually associated with a retinal
break (hole or tear) through which subretinal fluid (SRF) seeps and
separates the sensory retina from the pigmentary epithelium. This is
the commonest type of retinal detachment.
Traction retinal detachment
Tractionalretinal detachment (TRD) occurs due to retina being
mechanically pulled away from its bed by the contraction of fibrous
tissue in the vitreous .
Exudative (serous) retinal detachment occurs due to retina being
pushed away by neoplasm or accumulation of fluid beneath the retina
following inflammatory or vascular lesion
Exudative retinal detachment
10.
Clinical manifestations
• Sometimesthe first symptoms observed is transient flashes of light
(photopsia) in a particular part of visual field.
• Once a retinal break occurs there is release of pigment or a small
hemorrhage which manifest as floater or small moving spots in pts field
of vision .
• Once retinal detachment occurs curtains or veils obscuring the field of
vision.
• Pt experience fall in visual acuity when macula becomes detached or
large bullous detachment obstructs the fovea.
• Visual field loss occurs in the opposite quadrant of actual detachment.
12.
Diagnosis
• History andphysical examination
• Visual acuity measurement
• Opthalmoscopy
• Slit lamp microscopy
• Ultrasound of cornea,lens,or vitreous is hazy or opaque
13.
Management
• There isno known medical treatment for a detached retina. The goal
of surgical repair of retinal detachment is to place the retina back in
contact with the choroid and to seal the accompanying holes and
breaks.
1.Laser Photocoagulation
• If the retina is torn or the detachment is slight, a laser can be used to
burn the edges of the tear and halt progression. If the detachment is
small, the laser can seal the retina against the choroid. Laser surgery
is usually performed as an outpatient procedure under local
anesthesia.
14.
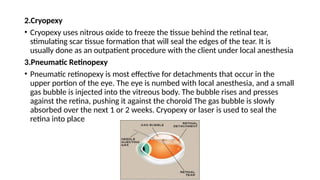
2.Cryopexy
• Cryopexy usesnitrous oxide to freeze the tissue behind the retinal tear,
stimulating scar tissue formation that will seal the edges of the tear. It is
usually done as an outpatient procedure with the client under local anesthesia
3.Pneumatic Retinopexy
• Pneumatic retinopexy is most effective for detachments that occur in the
upper portion of the eye. The eye is numbed with local anesthesia, and a small
gas bubble is injected into the vitreous body. The bubble rises and presses
against the retina, pushing it against the choroid The gas bubble is slowly
absorbed over the next 1 or 2 weeks. Cryopexy or laser is used to seal the
retina into place
15.
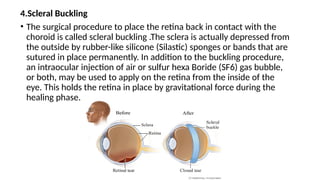
4.Scleral Buckling
• Thesurgical procedure to place the retina back in contact with the
choroid is called scleral buckling .The sclera is actually depressed from
the outside by rubber-like silicone (Silastic) sponges or bands that are
sutured in place permanently. In addition to the buckling procedure,
an intraocular injection of air or sulfur hexa Boride (SF6) gas bubble,
or both, may be used to apply on the retina from the inside of the
eye. This holds the retina in place by gravitational force during the
healing phase.
16.
Nursing management
• Helpingthe patient cope with fears and reality of loss of vision and to adapt to changes
in vision.
• Following surgery observe eye patch for any drainage ,assess pain and presence of
nausea .
• Activity restrictions may be necessary if an air or gas bubble has been injected .The
patient is placed usually head down and to one side so that bubble can apply maximum
pressure on retina.
• Postoperative eye medications generally antibiotic steroid combination eye drop to
prevent infection and inflammation. Cycloplegic agents –to dilate pupil and relax ciliary
muscles
• Instruct the client to clean eye with warm tap water using clean cloth .warm compress
can be continued at home .
• Advice to use eye glasses or shield .
• Advice to avoid vigorous exercise.






























![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


















