Downloaded 13 times




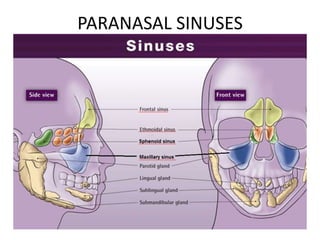






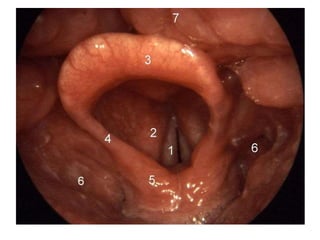


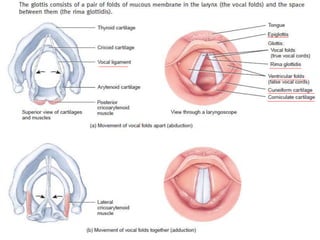














































This document provides information on the anatomy and physiology of the respiratory system. It describes the structures of the upper respiratory tract including the nose, pharynx, and larynx. It then discusses the lower respiratory tract including the trachea, bronchi, lungs, and alveoli. Key points include: - The nose functions to warm, moisten, and filter inhaled air, and contains paranasal sinuses. - The pharynx is a passageway for both air and food that connects to the larynx and esophagus. - The larynx contains vocal folds that vibrate to produce voice. Contraction of laryngeal muscles changes the tension of the vocal folds. - The trache





























































































