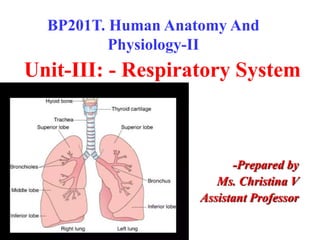
1. Unit-III: - Respiratory System
-Prepared by
Ms. Christina V
Assistant Professor
BP201T. Human Anatomy And
Physiology-II
2.
3. WHAT IS RESPIRATORY SYSTEM?
• The respiratory system (ventilatory system) is a
biological system, consisting of specific organs and
structures used for gas exchange in human.
• Organs of Respiratory System:
• Nose and nasal cavity.
• Pharynx
• Larynx
• Trachea
• Two bronchi
• Bronchioles
• Two Lungs
4.
5.
6.
7.
8.
9. RespiratorySystemFunctions
1. Supplies the body with oxygen and
disposes of carbon dioxide
2. Filters inspired air
3. Produces sound
4. Contains receptors for smell
5. Rids the body of some excess water and
heat
10. NOSE AND NASAL CAVITY
•POSITION AND STRUCTURE: Main route of air entry.
Two cavities divided by a SEPTUM. Anteriorly
consist hyaline cartilage. The roof is formed by
ethmoid bone.
The floor is formed by roof of the mouth. The
medial wall formed by the septum.
The lateral wall formed by the maxilla.
11.
12. RESPIRATORY FUNCTIONS OF THE
NOSE:
•The first of the respiratory passages.
•Warming-
Due to the immense vascularity of the
mucosa.
•Filtering and cleaning-
This occurs due to hairs which trap larger
particles.
•Humidification -
As air travels over the moist mucosa, it
becomes saturated with water vapor.
13.
14. PHARYNX
• What is pharynx?
The pharynx is the part of the throat that is behind
the mouth and nasal cavity and above the
esophagus and the larynx.
Length:- 12-14cm (extends from the base of the
skull to the level of 6th cervical vertebra.)
Position
Superiorly (higher)-Base of the skull.
Inferiorly (lower)-Continuous with the esophagus.
Anteriorly (towards)-Incomplete wall because of
the nose, mouth and larynx opening.
Posteriorly (behind)- Areolar tissue & first 6
vertebra.
15.
16. • For descriptive purposes the pharynx is
divided into three parts:
(i)The nasopharynx (ii)The oropharynx
(iii) The laryngopharynx
• (i) The nasopharynx
The nasal part of the pharynx lies behind the
nose.
• (ii)The oropharynx
The oral part of the pharynx lies behind the
mouth.
• (iii) The laryngopharynx
The laryngeal part of the pharynx extends from
the oropharynx.
17.
18. Functions
• Passageway for air and food.
• Warming and humidifying.
• Taste.
There are olfactory nerve endings.
• Protection.
The lymphatic tissue of the pharyngeal tonsils
produces antibodies.
• Speech.
Act as a resonating chamber for sound ascending
from the larynx.
19. LARYNX
• POSITION
• The larynx or voice box extends from the root of the
tongue.
• It lies in front of the laryngopharynx at the level of 3rd ,
4th ,5th and 6th cervical vertebra.
• Until the puberty there is little difference in the size of
the larynx between the male and female.
• It grows larger in the male.
Superiorly-The hyoid bone & roof of the tongue.
Inferiorly-Continuous with the trachea.
Anteriorly-The muscle of the neck.
Posteriorly-The laryngopharynx and 3rd to 6th cervical
vertebra.
20.
21.
22.
23.
24.
25.
26. STRUCTURE
•The larynx is composed of several irregularly shaped
cartilages attached to each other by ligaments and
membranes.
•The main cartilages are: 1 thyroid cartilage
- elastic fibrocartilage
2 arytenoid
cartilage:
epiglottis
The thyroid cartilage
This is the most prominent & consists of 2 flat pieces of
hyaline cartilage & fused anteriorly.
27. • The arytenoid cartilages
These are two roughly pyramid-shaped hyaline
cartilages situated on top of the broad part of the
cricoid cartilage.
• The epiglottis
This is a leaf-shaped fibroelastic cartilage attached
to the inner surface of the anterior wall of the
thyroid cartilage.
Blood and nerve supply
• Superior and inferior laryngeal arteries.
• Thyroid veins.
• Superior laryngeal nerves.
28. FUNCTIONS
•Production of sound
•Speech
•Protection of the lower respiratory tract
During swallowing the larynx moves
upwards and hinged epiglottis closes over the
larynx.
•Passageway for air
•Humidifying
•Filtering
•Warming
29.
30. TRACHEA
• Position
• The trachea or windpipe is a continuation of
the larynx & extends downwards to about the
level of T-5 where it divides into right & left
primary bronchi.
• Length-10-11cm
• Relation
Superiorly-the larynx
Inferiorly-the right & left bronchi
Anteriorly-upper part-the thyroid gland.
lower part-the arch of aorta & the sternum.
Posteriorly-.the oesophagus
Laterally- the lungs
38. BRONCHI & BRONCHIOLES:
• The two primary bronchi when the trachea divides about
the level of T-5.
• The right bronchus
• This is wider, shorter and more vertical than the left
bronchus.
• Length-2.5cm
• After entering the right lung, it divides into 3 branches, one
to each lobe.
• The left bronchus
• This is narrower than the right
• Length-5cm
• After entering the left lung, it divides into 2 branches, one
to each lobe.
39.
40.
41.
42. FUNCTIONS
•Control of air entry
•Warming & humidifying
•Support & patency
•Removal of particulate
matter
•Cough reflex
43. • RESPIRATORY BRONCHIOLES & ALVEOLI
• Each lobule is supplied with air by a terminal
bronchiole
• Which further subdivides into respiratory
bronchioles, alveolar ducts and large numbers of
alveoli (air sacs)
• About 150 million alveoli in the adult lung
• In these structures that the process of gas exchange
occurs.
• As airways progressively divide & become smaller &
smaller, their walls gradually become thinner.
• These distal respiratory passages are supported by a
loose network of elastic connective tissue.
• Exchange of gases in the lungs takes place in alveoli
44.
45. • FUNCTIONS
• External respiration
This is exchange of gases by diffusion between the
alveoli and the blood.
• Defense against microbes
Protective cells present within the lung tissue,
include lymphocytes & plasma cells, which
produce antibodies.
• Exchange of gases
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57. LUNGS
• There are two lungs,one lying on each side.
• Shape-cone
• Weight-600-700gms
• Length-20-24cm
• Colour-pinkish
• Lobes- three lobes in the right lung
two lobes in the left lung
• Lobes are separate by the fissures
• The area between the lungs is the
mediastinum.
58. • Surfaces
Apex A base
Costal surface
Medial surface
• Apex – rounded and rises into the root of the neck.
• A base-this is concave & semilunar in shape, lies on the
thoracic surface of the diaphragm.
• Costal surface-this surface is convex & lies against the costal
cartilages.
• Medial surface-this surface is concave & has a roughly
triangular-shaped area, called the hilum. The pulmonary
artery supplying the lung & two pulmonary veins draining it.
59.
60.
61. Pleura
• The pleura consists of a closed sac of serous
membrane, one for each lung which contains a small
amount of serous fluid.
• The lung is invaginated or pushed into this sac.
• It forms two layers: (i)The visceral pleura (ii)The
parietal pleura
• (i)The visceral pleura
This is adherent to the lung, covering each lobe &
passing into the fissures that separate them.
• (ii)The parietal pleura
This is adherent to the inside of the chest wall & the
thoracic surface of the diaphragm.
62. The pleural cavity
•The two layers of pleura are separated by a
thin film of serous fluid which allows them to
glide over each other.
•Preventing friction between them during
breathing.
•The serous fluid is secreted by the epithelial
cells of the membrane.
63.
64. RIGHT LUNG
•The right lung has more lobes and segments than
the left.
•It is divided into three lobes:
•
•
•
(i) Upper or superior lobe
(ii) Middle lobe
(iii) Lower or inferior lobe
• They separate by two fissures
• (i) One oblique fissure which separates
middle & lower lobe
• (ii) One horizontal fissure which separates
middle & upper lobe
65. LEFT LUNG
•The left lung is divided into two lobes
•(i) upper lobe
•(ii) lower lobe
•They separate by the oblique fissure
•Left lung does not have a middle lobe
•The mediastinal surface of the left lung has a
large cardiac impression or cardiac notch
where the heart sits.
67. FUNCTION
•Control of air entry
•Warming & humidifying
•Support & patency
•Removal of particulate
matter
•Cough reflex
68. RESPIRATION
• The term respiration means the exchange of
gases between body cells and the
environment.
• Breathing or pulmonary ventilation
• This is movement of air into and out of the
lungs.
• Exchange of gases:
• This takes place:
• In the lungs: external respiration.
• In the tissues: internal respiration.
69. • Mechanism of Breathing:
• 1. Breathing (Pulmonary ventilation):
• The mechanism of breathing involves the inspiration and
expiration of air with the movement of the diaphragm and
intercostal muscles.
• During inhalation, external intercostal muscles contract.
• At the same time, the diaphragm contracts and flattens.
• These actions increase the volume of the thoracic (chest)
cavity, and the air (oxygen) is forced into the lungs.
• On the contrary, exhalation occurs when the thoracic cavity
is reduced, and the air (carbon dioxide) is expelled out
70.
71. • 2. External Respiration:
• It involves the diffusion of oxygen and carbon dioxide
between the alveoli and the pulmonary capillaries due to the
partial pressure difference.
• The solubility of oxygen in the blood is not high, hence there
is a big difference in the partial pressure of oxygen in the
alveoli versus in the blood of the pulmonary capillaries.
• The partial pressure of oxygen in the alveoli is about
104mmHg, and it is about 40mmHg in the capillary blood.
• The difference is about 64mmHg
• This strong pressure gradient forces oxygen from the alveoli
into the blood across the respiratory membrane.
72. • 3. Internal Respiration:
• The gaseous exchange process that takes place in the
tissues is called internal respiration.
• The oxygen after dissociating from the hemoglobin
reaches the tissues or cells.
• The oxygen causes the complete breakdown of the
glucose molecules (food) into carbon, water, and
energy.
• The energy remains stored in the form of ATP
(Adenosine Triphosphate) and is further utilized to
perform several living activities.
• This mechanism of internal respiration is also named
Cellular Respiration.
73. • 4. Transport of
Oxygen: Oxygen is
carried through the
blood from the
respiratory organs
to the different
tissues.
• Oxygen can be
carried in two
forms:
• 1. Through plasma
• 2. Through Red
Blood Cells (RBCs)
74. • 5. Transport of Carbon Dioxide: Carbon
dioxide is transported in the blood in the below-
mentioned three ways:
• 1. In dissolved state: About 5−7per cent of
carbon dioxide is transported, being dissolved
in the plasma of blood.
• 2. In the form of bicarbonate: Carbon dioxide
produced by the tissues diffuses passively into
the blood and passes into the red blood
corpuscles, where it reacts with water to form
carbonic acid (H2CO3)
• 3. In combination with the amine group of
protein: (carbaminohemoglobin)
75. Regulation of Respiration
• Respiration is
regulated by two
mechanisms:
• Nervous or neural
mechanism
• Chemical
mechanism.
76.
77. NERVOUS MECHANISM
• Respiratory centers, Afferent nerves and Efferent
nerves
• RESPIRATORY CENTERS: Respiratory centers are
group of neurons, which control the rate, rhythm and
force of respiration.
• These centers are bilaterally situated in brainstem.
• Depending upon the situation in the brainstem, the
respiratory centers are classified into two groups:
–Medullary centres
–Pontine centres
78. • Medullary centers, which are made up of:
o Dorsal respiratory group of neurons: basic rhythm of
respiration.
• Pontine centres which are:
o Pneumotaxic center:. Pneumotaxic center influences the
switching between inspiration and expiration.
o Apneustic center: The apneustic center increases the depth
of inspiration by acting directly on the dorsal group neurons.
o Apneusis is an abnormal pattern of respiration or breathing
irregularity characterized by prolonged inspiration followed
by short, inefficient expiration.
79. • Afferent Pathway:
• Impulses from peripheral chemoreceptors and baroreceptors
are carried to the respiratory centers by the branches of
glossopharyngeal and vagus nerves.
• Respiratory centers receive afferent impulses from different
parts of the body and, modulate the movements of thoracic
cage and lungs accordingly through efferent nerve fibers.
80. • Efferent Pathway:
• The nerve fibers from the respiratory centers leave
brainstem, descend in spinal cord, and terminate on the
motor neurons in the anterior horn cells of cervical and
thoracic segments of spinal cord.
• From the motor neurons of spinal cord, two sets of
nerve fibers arise:
• Phrenic nerve fibers (C3 – C5) which supply the
diaphragm
• The intercostal nerve fibers (T1 – T11) which supply the
external intercostal muscles
81. • Chemical control :
• The chemical regulatory mechanism adjusts ventilation
in such a way that the alveolar PCO2 is normally held
constant.
• The receptors in the carotid and aortic bodies are
stimulated by a rise in the PCO2 of the arterial blood.
82. Lung Volumes and Capacities
• Lung volumes, can be measured directly by
use of a spirometer
• Lungs capacities, are combinations of
different lung volumes.
• The apparatus used to measure volumes and
capacities is called a spirometer or
respirometer
• The record is called a spirogram.
83. Lung Volumes:
• While at rest, a healthy adult averages 12 breaths a minute,
with each inhalation and exhalation, moving about 500 mL
of air into and out of the lungs. The volume of one breath is
called the tidal volume (VT).
• Tidal volume (TV)- this is the amount of air passing into and
out of the lungs during each cycle of breathing. About 500ml
is tidal volume.
By taking a very deep breath, you can inhale a good deal
more than 500 mL. This additional inhaled air, called the
inspiratory reserve volume (IRV), is about 3100 mL in an
average adult male and 1900 mL in an average adult female
84. LUNG VOLUMES AND CAPACITIES
• Respiratory cycles-15/minute
• Tidal volume (TV)- this is the amount of air passing into and
out of the lungs during each cycle of breathing.
• About 500ml is tidal volume.
• EXCHANGE OF GASES
• Inhaled oxygen enters the lungs and reaches the alveoli.
The layers of cells lining the alveoli and the surrounding
capillaries are each only one cell thick and are in very close
contact with each other.
• Oxygen passes quickly through air-blood barrier into the
blood in the capillaries.
• Similarly, carbon dioxide passes from the blood into the
alveoli and is then exhaled.
85.
86. • If you inhale normally and then exhale as forcibly as
possible, you should be able to push out considerably
more air in addition to the 500 mL of tidal volume. The
extra 1200 mL in males and 700 mL in females is called
the expiratory reserve volume (ERV).
• The forced expiratory volume in 1 second, (FEV1) is the
volume of air that can be exhaled from the lungs in 1
second with maximal effort following a maximal
inhalation.
87. • Even after the expiratory reserve volume is exhaled,
considerable air remains in the lungs because the sub
atmospheric intrapleural pressure keeps the alveoli slightly
inflated, and some air remains in the noncollapsible airways.
This volume, which cannot be measured by spirometry, is
called the residual volume (re-ZID-u-al) (RV) and amounts to
about 1200 mL in males and 1100 mL in females.
• If the thoracic cavity is opened, the intrapleural pressure
rises to equal the atmospheric pressure and forces out some
of the residual volume. The air remaining is called the
minimal volume.
88. Lung Capacities:
• Inspiratory capacity (IC) is the sum of tidal volume and
inspiratory reserve volume (500 mL + 3100 mL = 3600 mL in
males and 500mL + 1900 mL = 2400 mL in females).
• Functional residual capacity (FRC) is the sum of residual
volume and expiratory reserve volume(1200 mL + 1200 mL =
2400 mL in males and 1100 mL + 700 mL =1800 mL in
females).
• Vital capacity (VC) is the sum of inspiratory reserve volume,
tidal volume, and expiratory reserve volume (4800 mL in
males and 3100 mL in females).
• Total lung capacity (TLC) is the sum of vital capacity and
residual volume (4800 mL + 1200 mL =6000 mL in males and
3100 mL + 1100 mL = 4200 mL in females).
89. • The minute ventilation (V)—the total volume of air
inspired and expired each minute—is tidal volume
multiplied by respiratory rate. In a typical adult at
rest, minute ventilation is about 6000 mL/min (V= 12
breaths per minute × 500 mL = 6000 mL/min).
• The alveolar ventilation (VA) is the volume of air per
minute that actually reaches the respiratory zone
(350 mL). Alveolar ventilation is typically about 4200
mL/min (VA = 12 breaths per minute × 350 mL = 4200
mL/min).
91. Oxygen transport
The heme portion of haemoglobin
• 4 atoms of iron
• Each is capable of binding to a molecule of oxygen
Oxygen and Haemoglobin
• Forms oxyhaemoglobin (Hb + O2 = HbO2)
Oxygen and haemoglobin dissociation and binding factors
• The partial pressure of oxygen Po2
• Higher pressure, more binding
• Saturation
Fully oxidised – fully saturated
A mixture of Hb and HbO2 – partially saturated
Percent saturation of haemoglobin – average saturation of a
molecule with oxygen
High partial pressure = more binding until full saturation
92. • Factors affecting oxygen’s affinity for hemoglobin:
1. Acidity
Decrease in pH affinity of hemoglobin for oxygen decreases
• Dissociation curve shifts to right
• Oxygen dissociates from haemoglobin
• Bohr Shift effect
Elevated pH affinity-Dissociation curve shifts to the left
2. Partial pressure of carbon dioxide
• Co2 can bind to Hb
• Decreased partial pressure of carbon dioxide shifts dissociation curve to the
left
3. Temperature
• High temp= more dissociation of O2 from Hb
4. 2,3-Bisphosphoglycerate (BPG)
• Previously called DPG
• Decreases affinity of hemoglobin for oxygen and helps unload oxygen from
hemoglobin
When combined with hemoglobin, the hemoglobin binds less tightly to oxygen
93. Carbon dioxide transport
• In a resting person, metabolism generates about 200
ml of CO2 per minute.
• This CO2 is transported to the lungs from the tissues
by the blood in three ways-
a) As dissolved gas – about 10% of CO2 entering the
blood remains physically dissolved in plasma and carried
as such.
b) As carbamino Hb- about 30% of CO2 reacts with Hb to
form carbamino Hb and is transported to the lungs
94.
95.
96. BREATHING
• Breathing supplies oxygen to the alveoli, and
eliminates carbon dioxide.
• MUSCLES OF BREATHING
• Expansion of the chest during inspiration
occurs as a result of muscular activity, partly
voluntary and partly involuntary.
• The main muscles used in normal quiet
breathing are the INTERCOSTAL MUSCLES and
the DIAPHRAGM.
• During difficult or deep breathing they are
assisted by muscles of the neck, shoulders
and abdomen.
97. INTERCOSTAL MUSCLES
•There are 11 pairs of intercostal muscles that
occupy the spaces between the 12 pairs of
ribs.
•They are arranged in two layers, the external
and internal intercostal muscles
•The first rib is fixed.
•Therefore, when the intercostal muscles
contract they pull all the other ribs towards
the first rib. Because of the shape and sizes of
the ribs they move outwards when pulled
upwards, enlarging the thoracic cavity.
98.
99. DIAPHRAGM
•The diaphragm is a dome-shaped muscular
structure separating the thoracic and abdominal
cavities.
•It forms the floor of the thoracic cavity and the
roof of the abdominal cavity and consists of a
central tendon from which muscle fibers radiate to
be attached to the lower ribs and sternum and to
the vertebral column by two crura.
•When the muscle of the diaphragm is relaxed ,the
central tendon is pulled downwards to the level of
the T-9,enlarging the thoracic cavity in length.
•This decreases pressure in the thoracic cavity and
increases it in the abdominal and pelvic cavities.
100.
101. • The intercostal muscles and the diaphragm
contract simultaneously, enlarging the
thoracic cavity in all directions.
• CYCLE OF BREATHING
• The average respiratory rate is 12 to 15
breaths/minute.
• Each breath consists of three phases:
• (i)Inspiration
• (ii)Expiration
• (iii)Pause.
102. (i)Inspiration
When the capacity of the thoracic cavity is increased
by simultaneous contraction of the intercostal
muscles and the diaphragm.
• The parietal pleura moves with the walls of the
thorax & the diaphragm.
• This reduces the pressure in the pleural cavity to a
level considerably lower than atmospheric pressure.
• The visceral pleura follows the parietal pleura, pulling
the lungs with it.
• This expands the lungs and the pressure within the
alveoli and in the air passages, drawing air into the
lungs in attempt to equalize the atmospheric and
alveolar air pressure.
103. • The process of inspiration is ACTIVE, as it needs
energy for muscle contraction.
• Inspiration lasts about 2 seconds.
• (ii)Expiration
• Relaxation of the intercostal muscles and the
diaphragm results in downward and inward
movement of the rib cage and elastic recoil of the
lungs.
• As this occurs, pressure inside the lungs exceeds
that in the atmosphere and so air is expelled from
respiratory tract.
• The still contain some air, are prevented from
collapse by the intact pleura.
• This process is PASSIVE as it does not require the
expenditure of energy.
107. CARDIOPULMONARY RESUSCITATION (CPR)
• Cardiopulmonary resuscitation (CPR) consists of the
use of chest compressions and artificial ventilation to
maintain circulatory flow and oxygenation during
cardiac arrest .
7 STEPS OF CARDIOPULMONARY RESUSCITATION:
• 1. Checking the scene and the person
• 2. Call for help /assistance
• 3. Opening the airway
• 4. Checking for breathing.
• 5. Chest compressions
• 6. Delivering rescue breaths
• 7. Repeating CPR steps
108.
109.
110. Mouth-to-mouth Resuscitation:
• This is an effective method of introducing air
into the victim’s lungs if the victim has
stopped breathing but still has pulse.
• Methods of administering mouth-to-mouth
resuscitation
• Place the victim on his back. Loosen his shirt
around the neck.
112. • Open his mouth and sweep or hook finger
deep inside to remove any debris
• (blood, knocked teeth, dentures, etc.).
113. Hold the back of the neck with one hand. Place the heel
of your other hand on is forehead and tilt his head as far
as you can.
•.
114. •Using the hand on his forehead, pinch the
nostrils. Take a deep breath and open your
mouth. Seal it over his mouth and blow.
His chest will rise as the air is forced into
his lungs.
•If the victim is a child, cover his nose and
mouth with your mouth, but do not blow
as hard as you would for an adult. This is
also known as mouth-to-nose
resuscitation.
115. •Wait for the victim’s chest to fall,
then repeat the process. Do it two
(2) times in quick succession.
•Continue mouth-to-mouth
resuscitation steadily at the rate of
12-20 breaths per minute, until the
victim (adult) starts breathing or
until medical help comes.
116. •Once the victim is breathing normally, put him
in a recovery position.