Downloaded 177 times


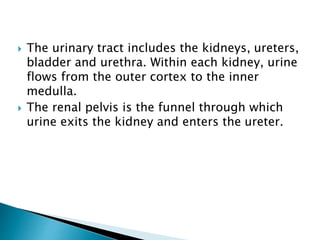
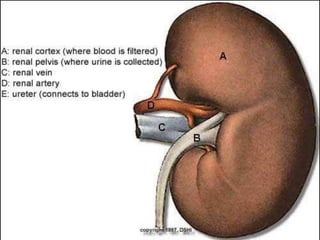
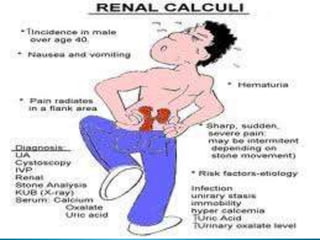



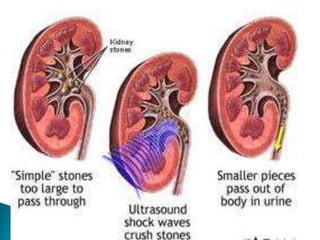

The document discusses urinary tract stones (calculi) including their formation, types, symptoms, diagnosis, and treatment. Key points: - Stones form when urinary concentrations of minerals like calcium, oxalate, and uric acid increase. - Symptoms include sharp pain (renal colic) radiating from the back to the groin as stones pass through the urinary tract. - Diagnosis involves imaging tests like CT scans, X-rays, and ultrasounds to detect radiopaque stones. - Treatment depends on stone size but may include shock wave lithotripsy, ureteroscopy, or open surgery to remove stones. Recurrence rates after treatment remain high.





![Interstitial cystitis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/interstitialcystitis1-150315053919-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)


























































![Urolithiasis presented by Dr Muhammad nouman([Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/urolithiasisautosaved-1-250603143258-c924c676-thumbnail.jpg?width=640&height=640&fit=bounds)






















