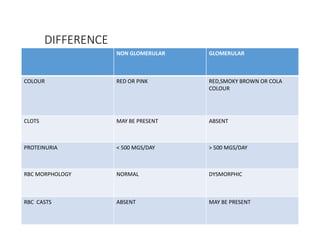
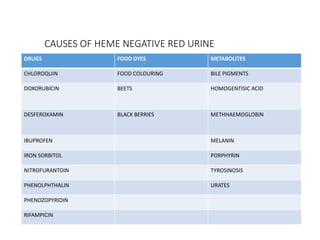
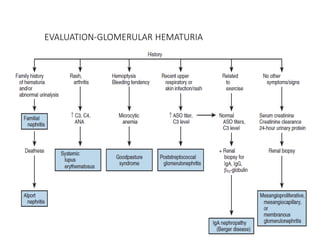
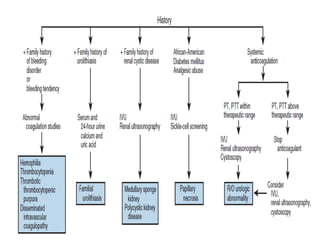
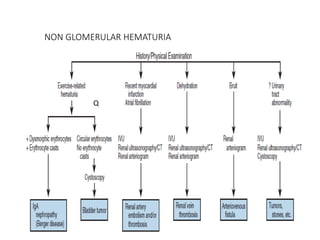
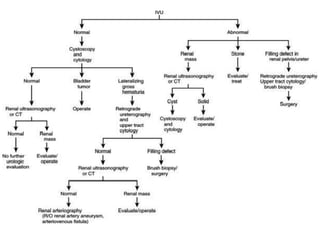
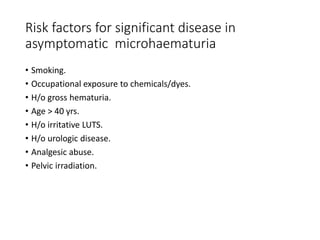
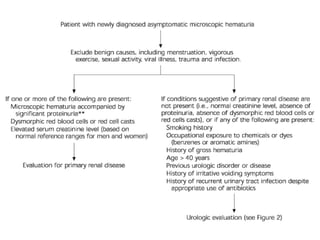
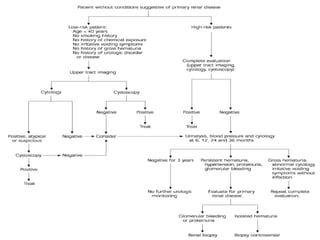
The document discusses hematuria, including its definition, classification (microscopic vs. gross), and various causes, with a focus on glomerular and non-glomerular origins. It emphasizes the importance of evaluation, including history taking, laboratory tests, and imaging techniques to differentiate between types of hematuria and assess potential underlying conditions. Additionally, it highlights treatment options for intractable hematuria and the need for careful follow-up and monitoring of patients.