Downloaded 58 times
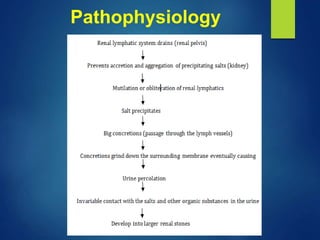
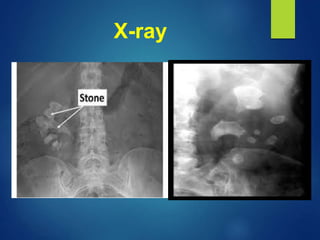
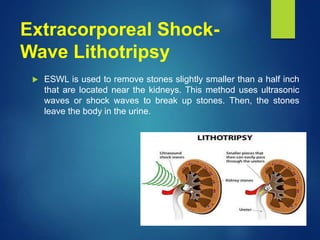
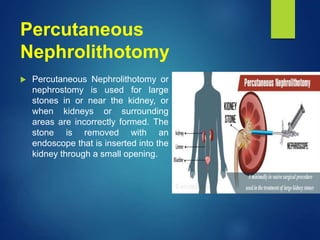
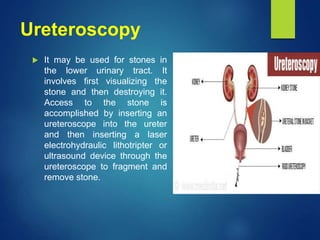
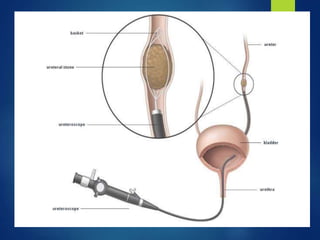


Renal stones, also known as kidney stones, form in the urinary tract and can affect any part from the kidneys to the bladder. Risk factors include metabolic abnormalities, warm climates, certain diets, genetics, and lifestyle. The five major types of renal stones are calcium phosphate, calcium oxalate, uric acid, cysteine, and struvite. Symptoms include severe side and back pain, painful urination, hematuria, and nausea. Diagnostic tests include imaging like ultrasounds and CT scans as well as urine and blood tests. Treatment options depend on the size and location of the stone and include shockwave lithotripsy, percutaneous nephrolithotomy, ureter























































































