- Extracorporeal shockwave lithotripsy (ESWL) uses shockwaves to fragment kidney stones noninvasively. It was discovered in the 1980s during military research.
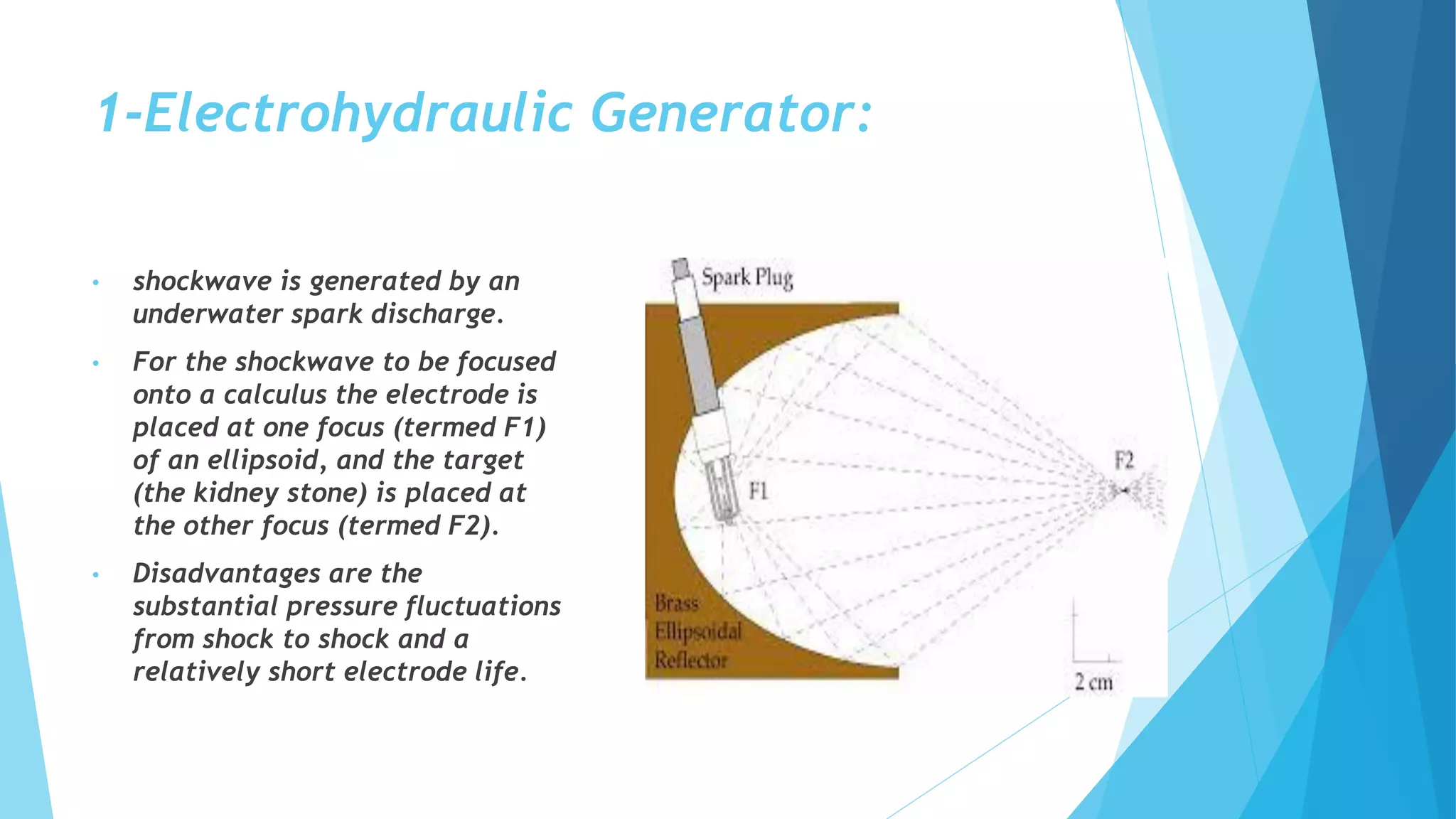
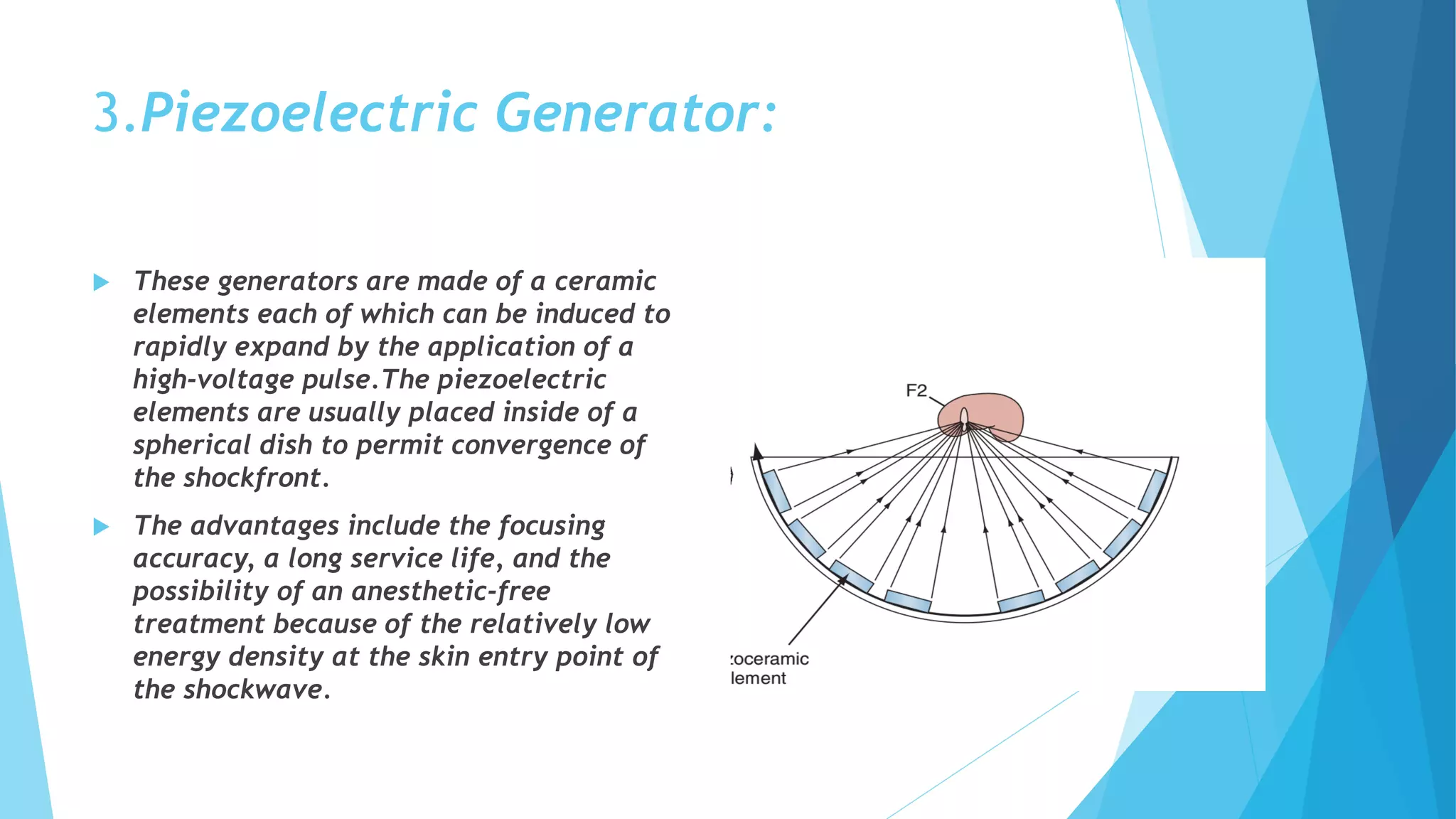
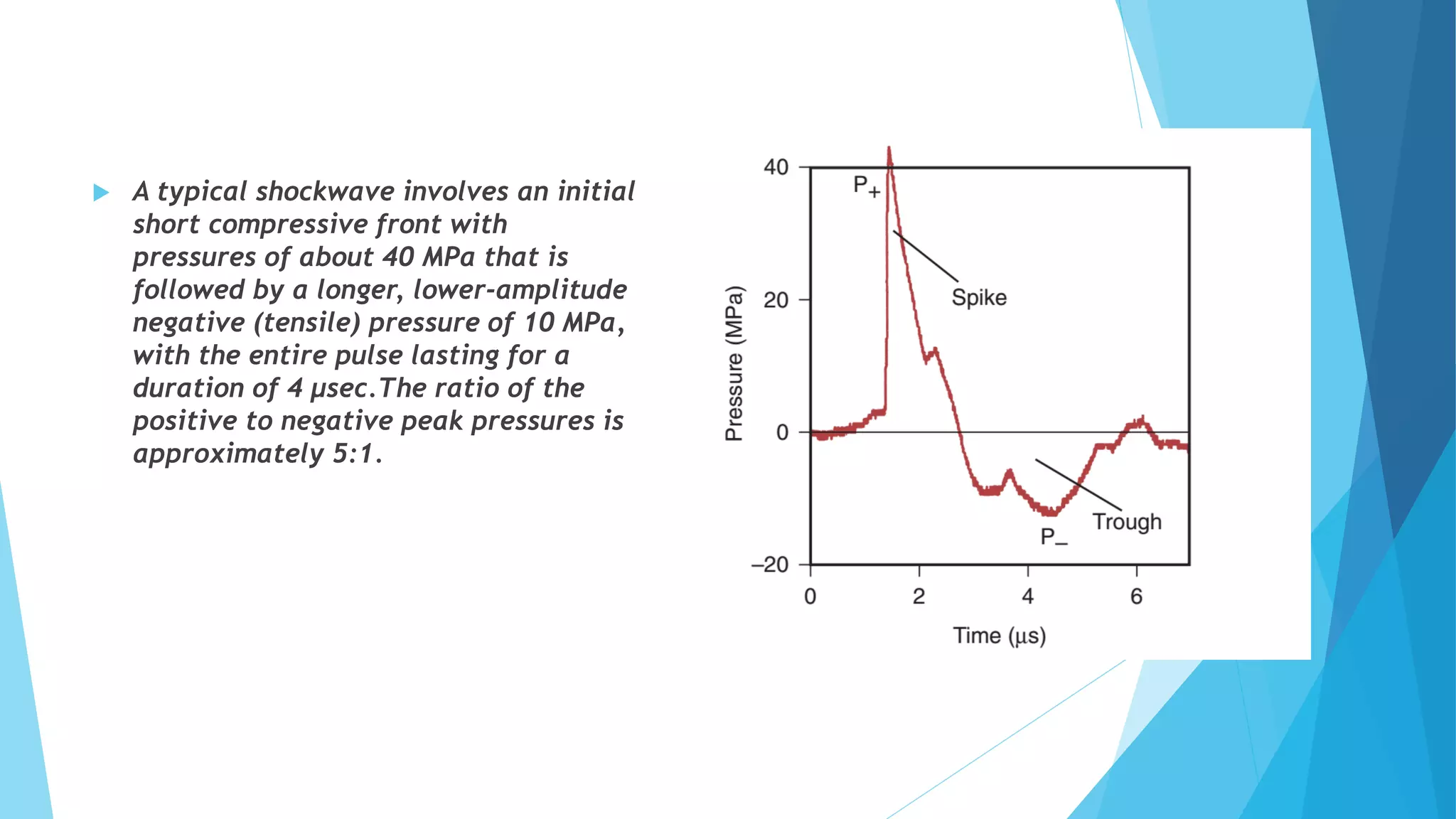
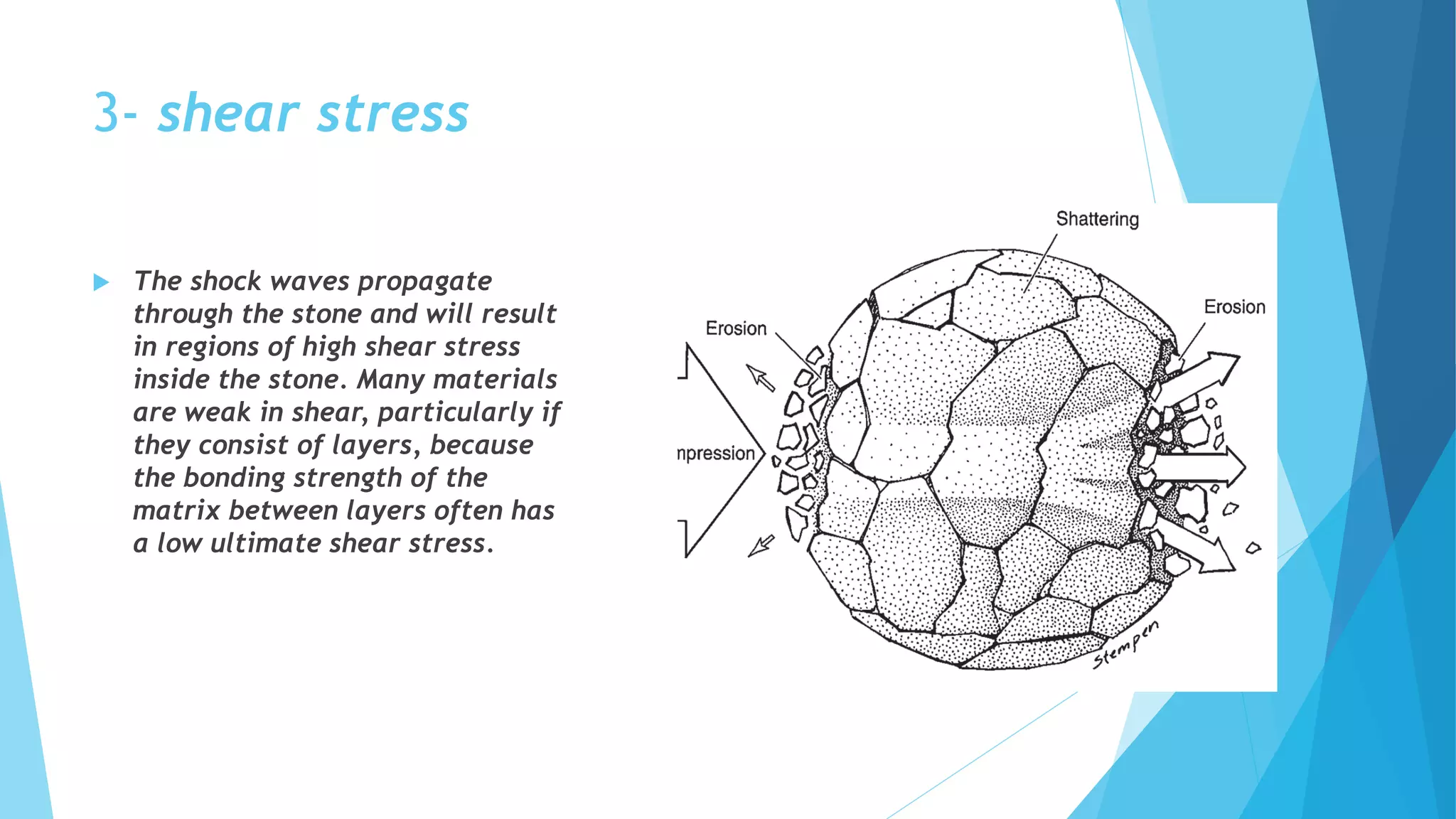
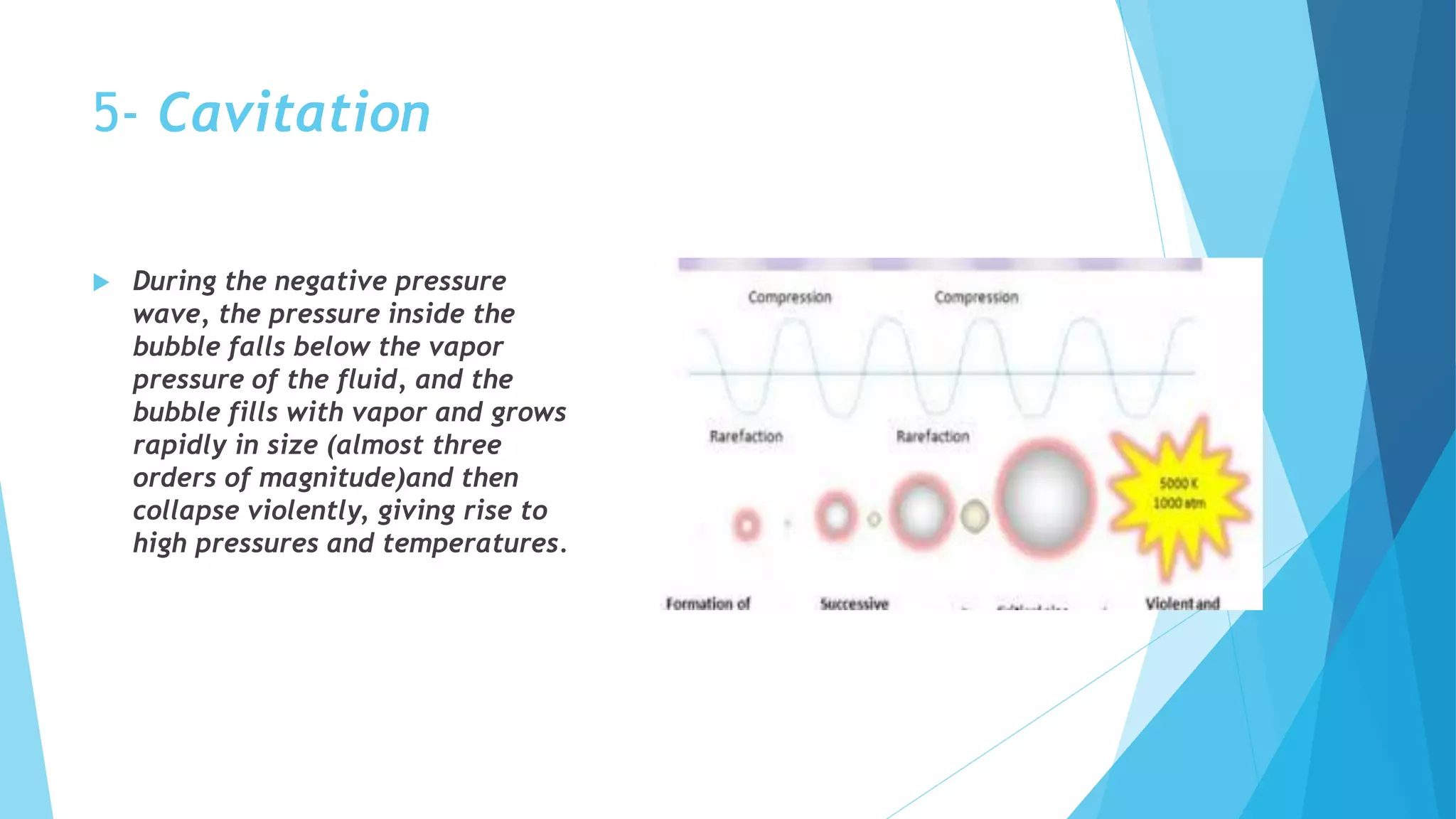
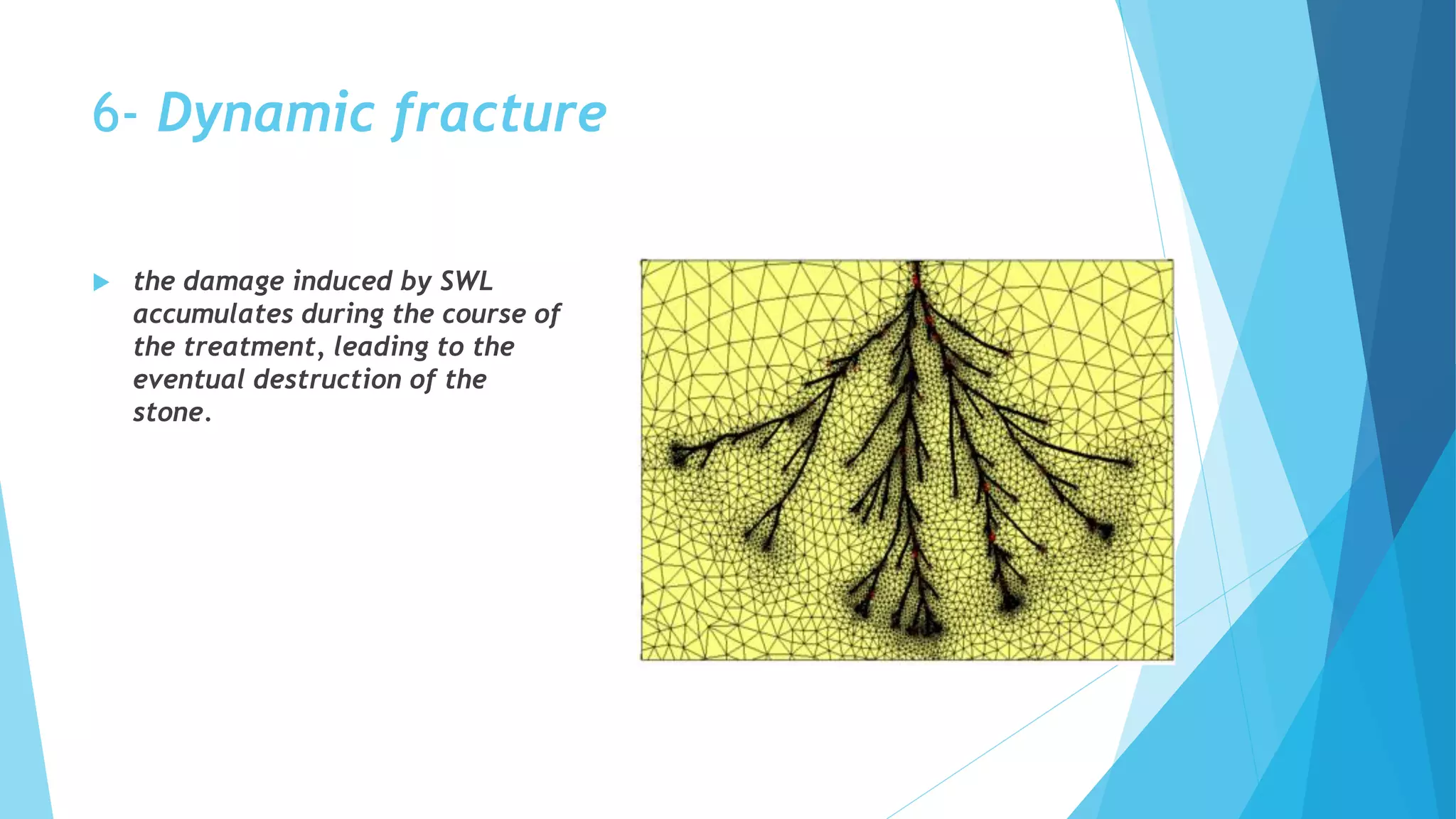
- ESWL uses different generators (electrohydraulic, electromagnetic, piezoelectric) to focus shockwaves on stones. Ultrasound and fluoroscopy are used for imaging. Stone fragmentation occurs through mechanisms like spall fracture and squeezing.
- While usually low risk, ESWL can potentially cause acute extrarenal or renal injuries. Chronic risks include higher blood pressure and stone recurrence. Techniques like adequate anesthesia and coupling aim to optimize outcomes.










































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


