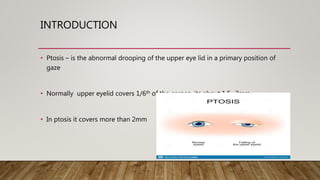
This document provides a comprehensive evaluation of ptosis, detailing its definition, classifications (congenital and acquired), history taking, examination methods, measurement techniques, grading, and surgical treatments. Key aspects include differentiating between true ptosis and pseudoptosis, evaluating ptosis severity, and various diagnostic tests such as the ice test and tensilon test. The document concludes with references for further reading and documentation requirements for ptosis evaluations.