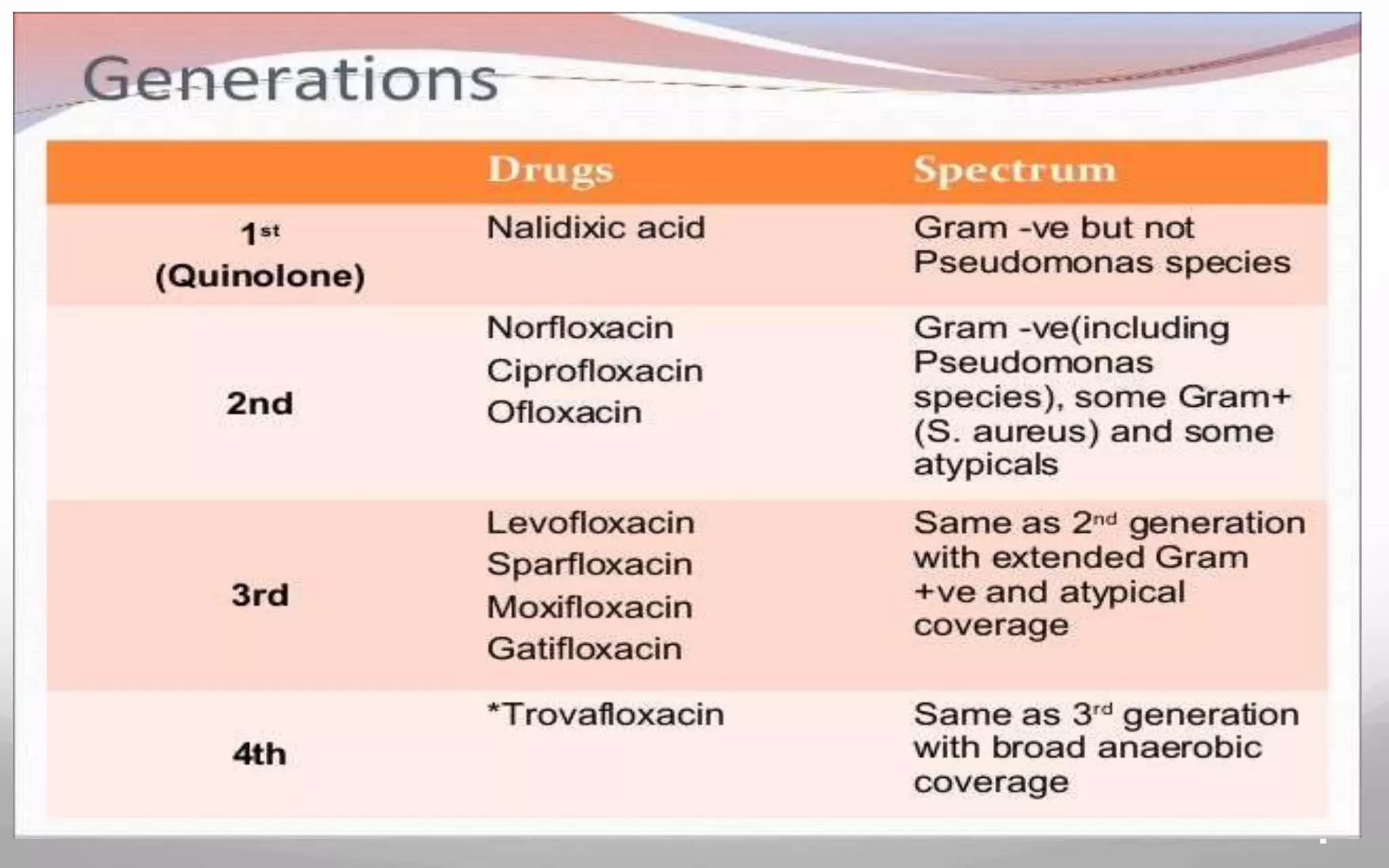
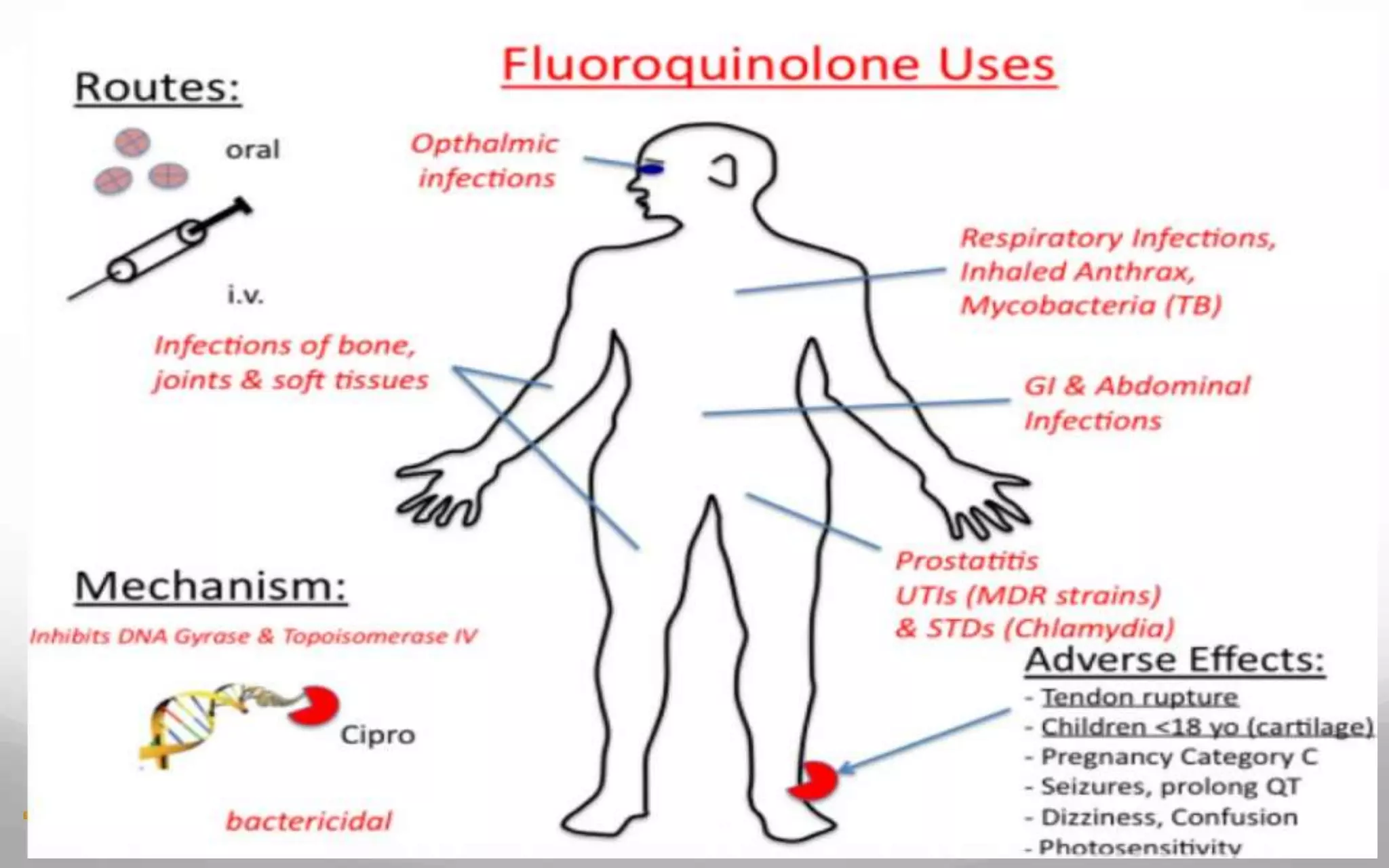
The document summarizes quinolones and fluoroquinolones, a family of broad-spectrum antibacterial agents. It discusses their mechanism of action, which involves inhibiting bacterial DNA gyrase and topoisomerase IV, blocking DNA synthesis. Common examples like ciprofloxacin, norfloxacin, ofloxacin, pefloxacin and levofloxacin are described in terms of their pharmacokinetics, therapeutic uses, doses, and adverse effects which include gastrointestinal issues and central nervous system effects. Mechanisms of resistance and drug interactions are also covered at a high level.