Download as PDF, PPTX






















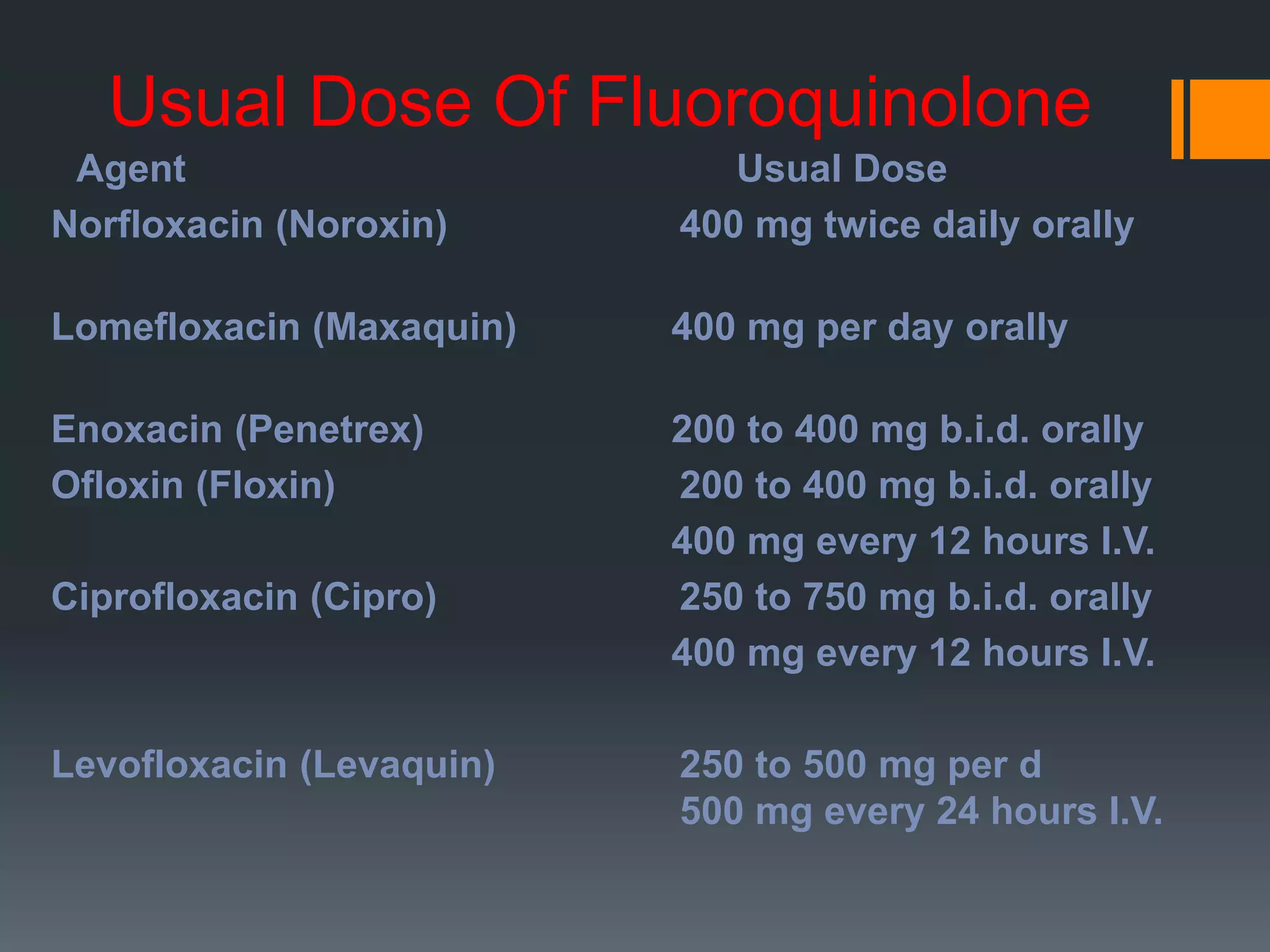
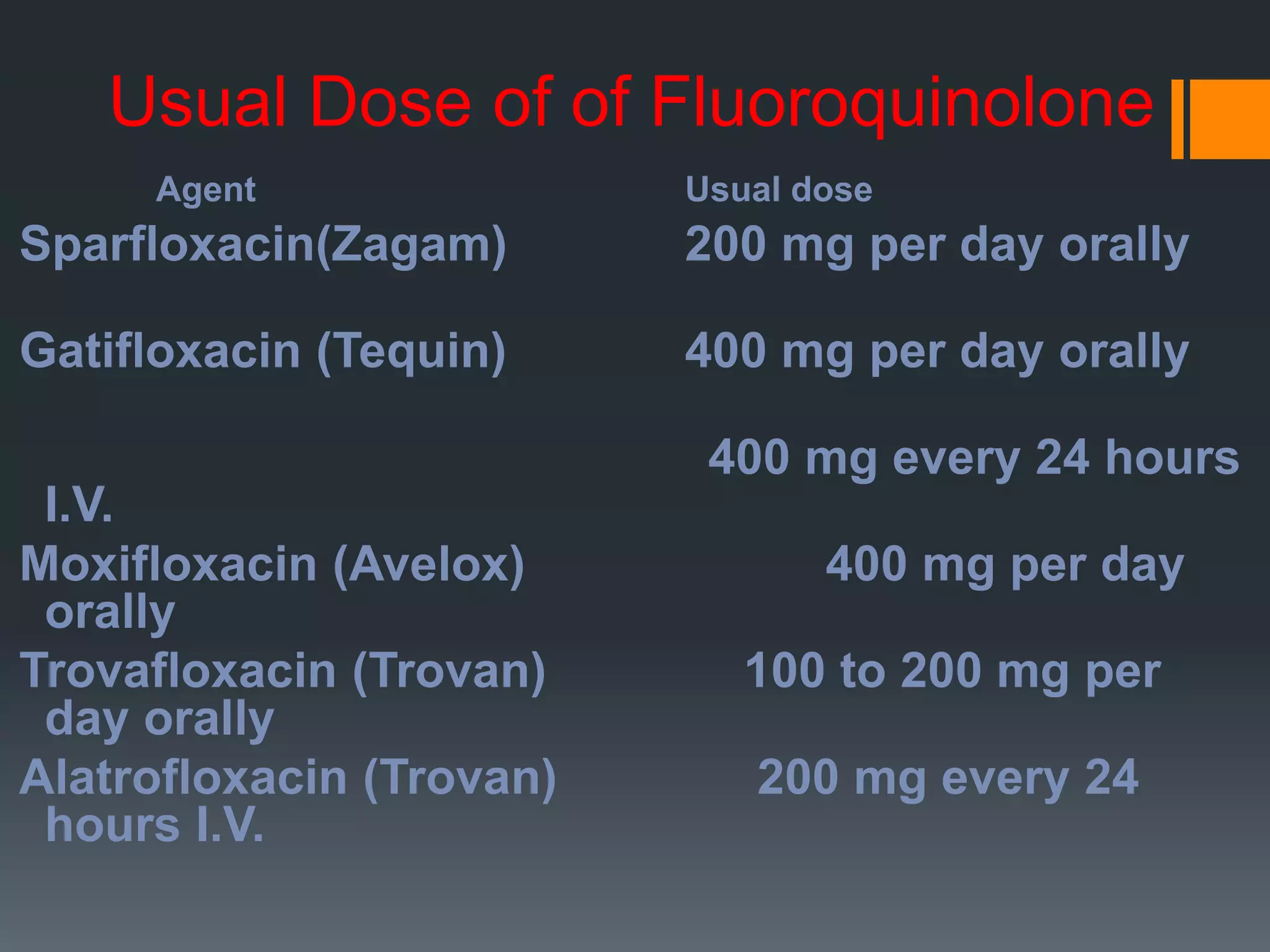


The document summarizes quinolones and fluoroquinolones. Quinolones are a family of synthetic broad-spectrum antibacterial drugs that prevent bacterial DNA from duplicating. Fluoroquinolones are derived from quinolones and have an even broader spectrum. They work by inhibiting bacterial DNA gyrase and topoisomerase, preventing DNA replication. First-generation quinolones targeted gram-negative bacteria, while later generations achieved broader coverage including some gram-positives and atypical bacteria. Fluoroquinolones are well-absorbed orally and penetrate tissues well, making them useful for various infections. However, resistance has emerged through mutations and efflux pumps.























































































