Downloaded 20 times

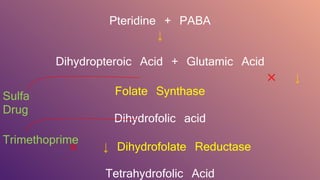

Cotrimoxazole is a fixed-dose combination of trimethoprim and sulfamethoxazole, introduced in 1969, that inhibits bacterial folate metabolism and is effective in treating various infections. The combination is synergistic, providing a cidal effect against many organisms, and is particularly effective for infections caused by bacteria that are resistant to either component alone. However, cotrimoxazole can cause adverse effects similar to sulfonamides and should be used cautiously in specific populations, including pregnant women and those with renal impairment.






































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
















