Downloaded 189 times


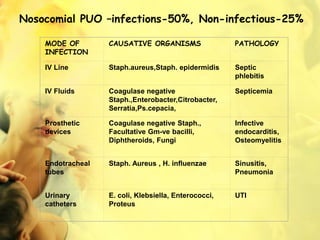













Pyrexia of unknown origin (PUO) is defined as a fever over 38°C lasting three weeks or longer without a diagnosis despite extensive investigation. There are various types of PUO, including classic, nosocomial, neutropenic, and HIV-associated, each with specific characteristics and diagnostic criteria. Effective management requires thorough diagnostic workup and ideally should delay therapy until the cause is identified to ensure the correct treatment.







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















