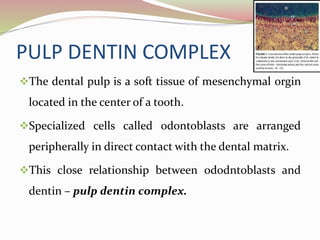
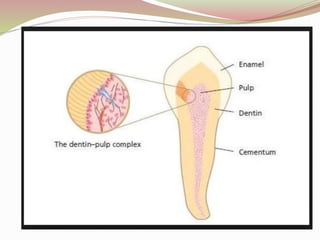
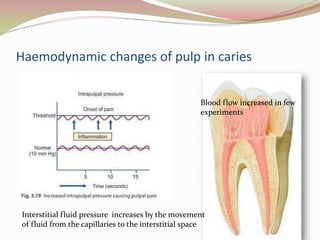
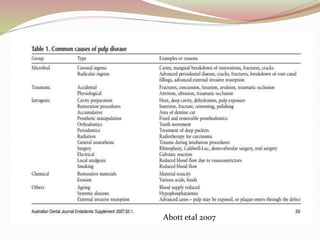
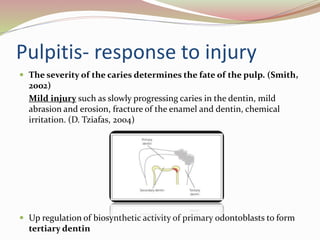
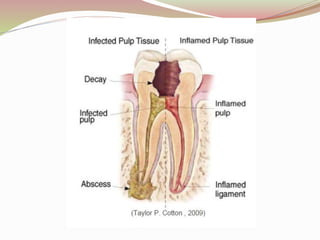
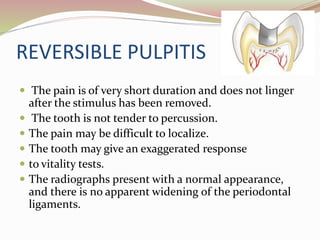
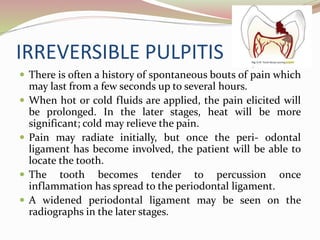
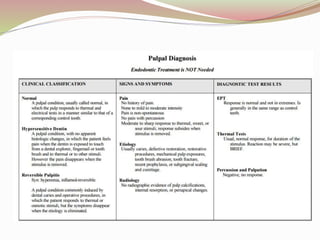
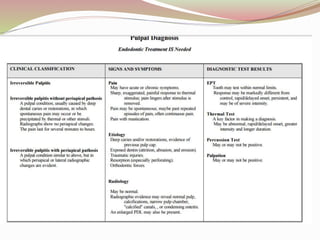
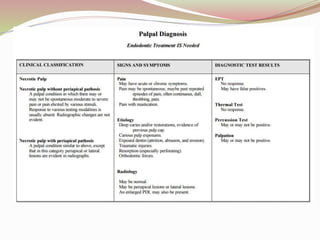
The dental pulp is a soft tissue located within the center of a tooth that is surrounded by rigid dental structures. It contains blood vessels and nerves that make it highly sensitive. When bacteria enter through decay or cracks, they can cause inflammation of the pulp, known as pulpitis. Pulpitis can be reversible if caught early through mild symptoms like short pain from hot and cold. But over time, the inflammation can become irreversible as the bacteria spread, causing spontaneous, lingering pain that is worse when lying down and radiates elsewhere. This damages the pulp irreversibly.
































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

