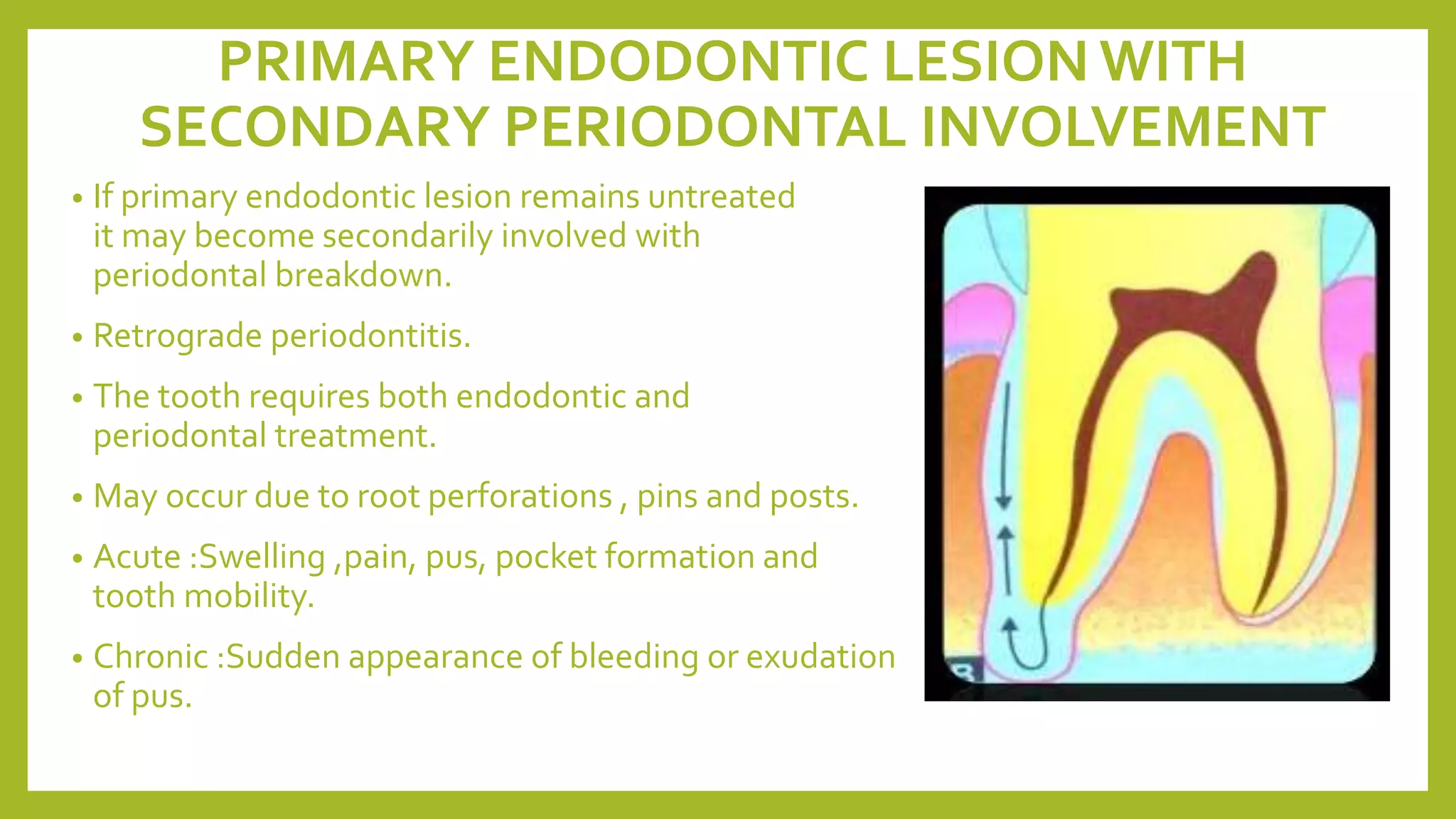
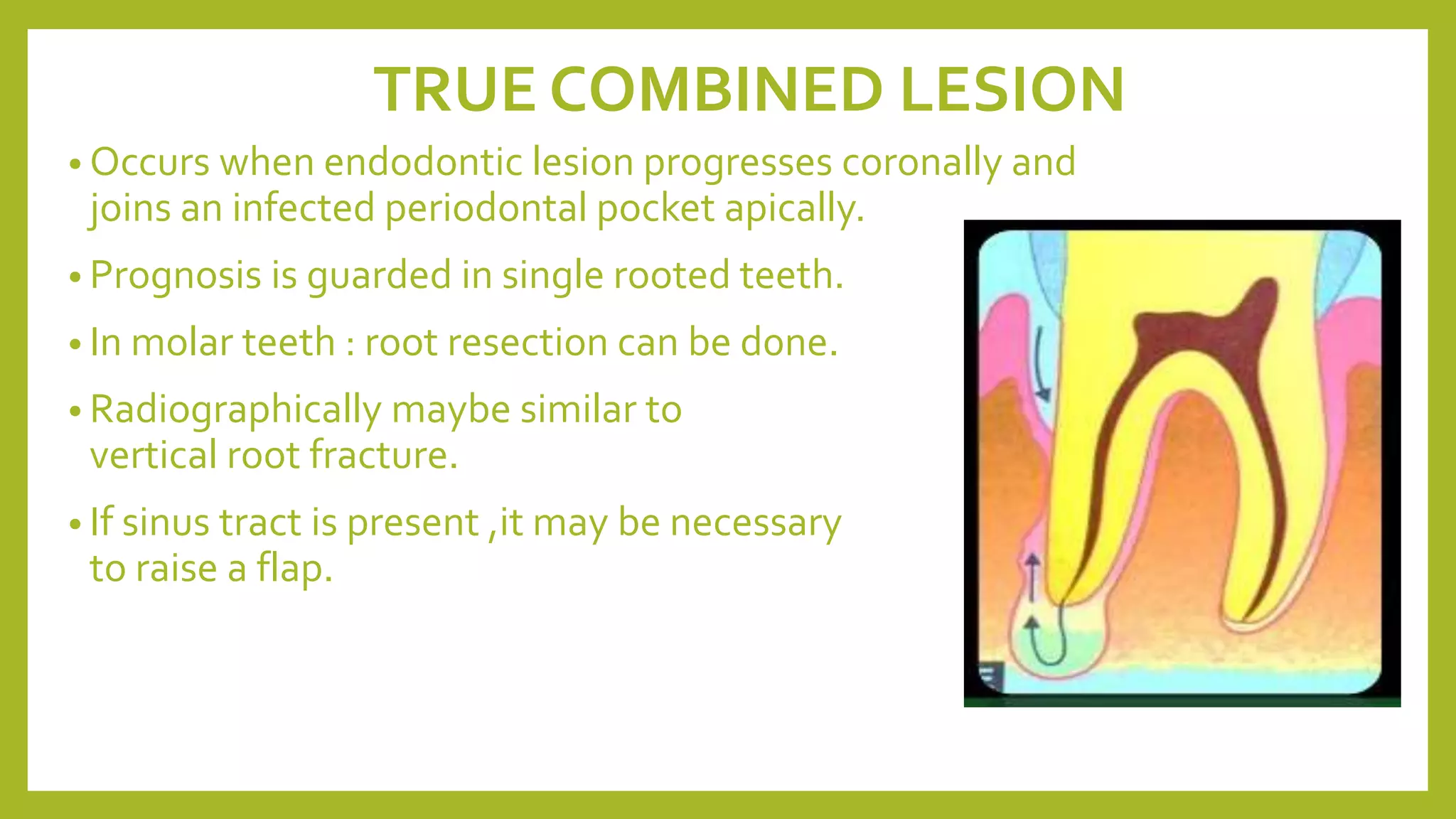
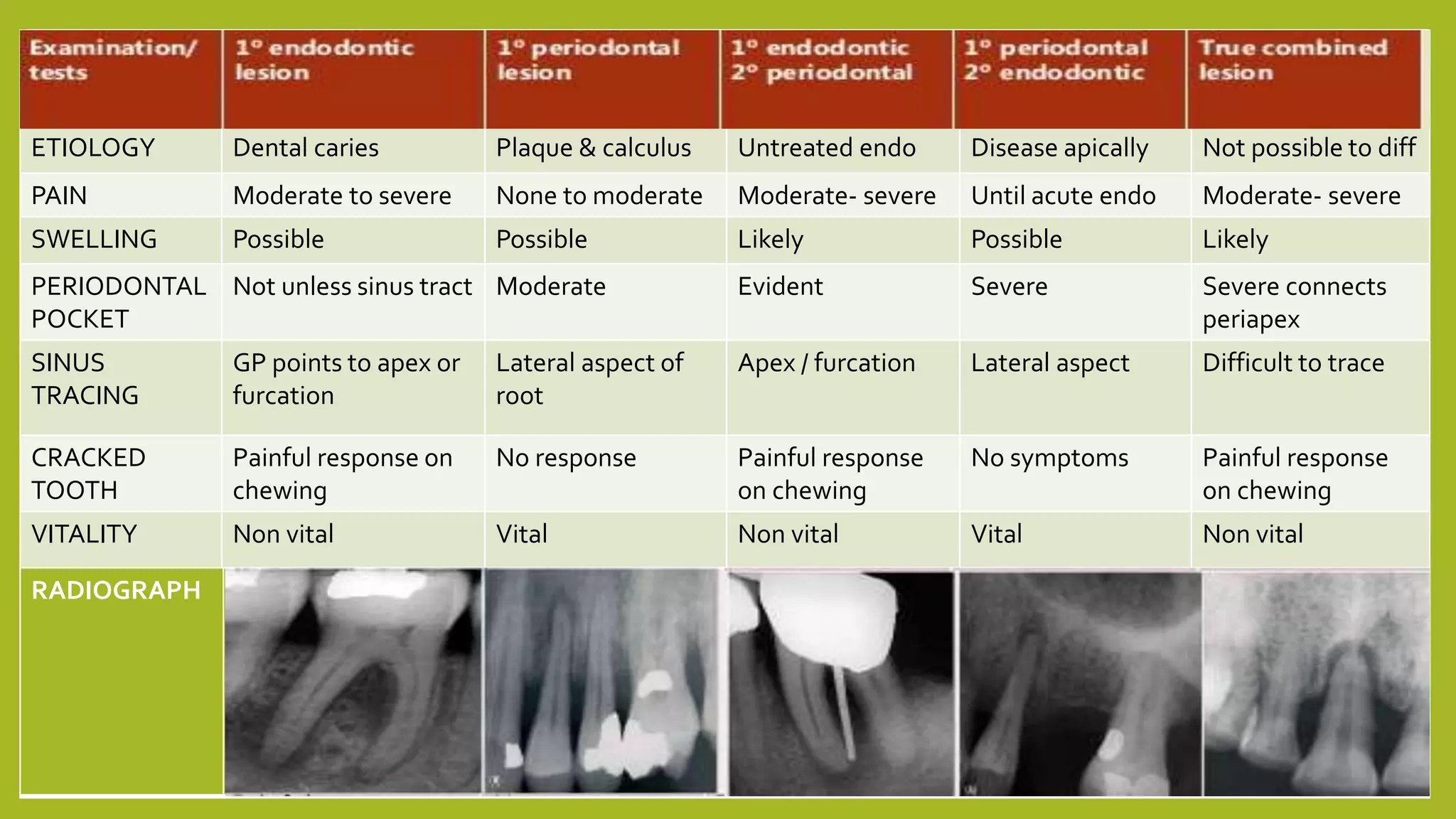
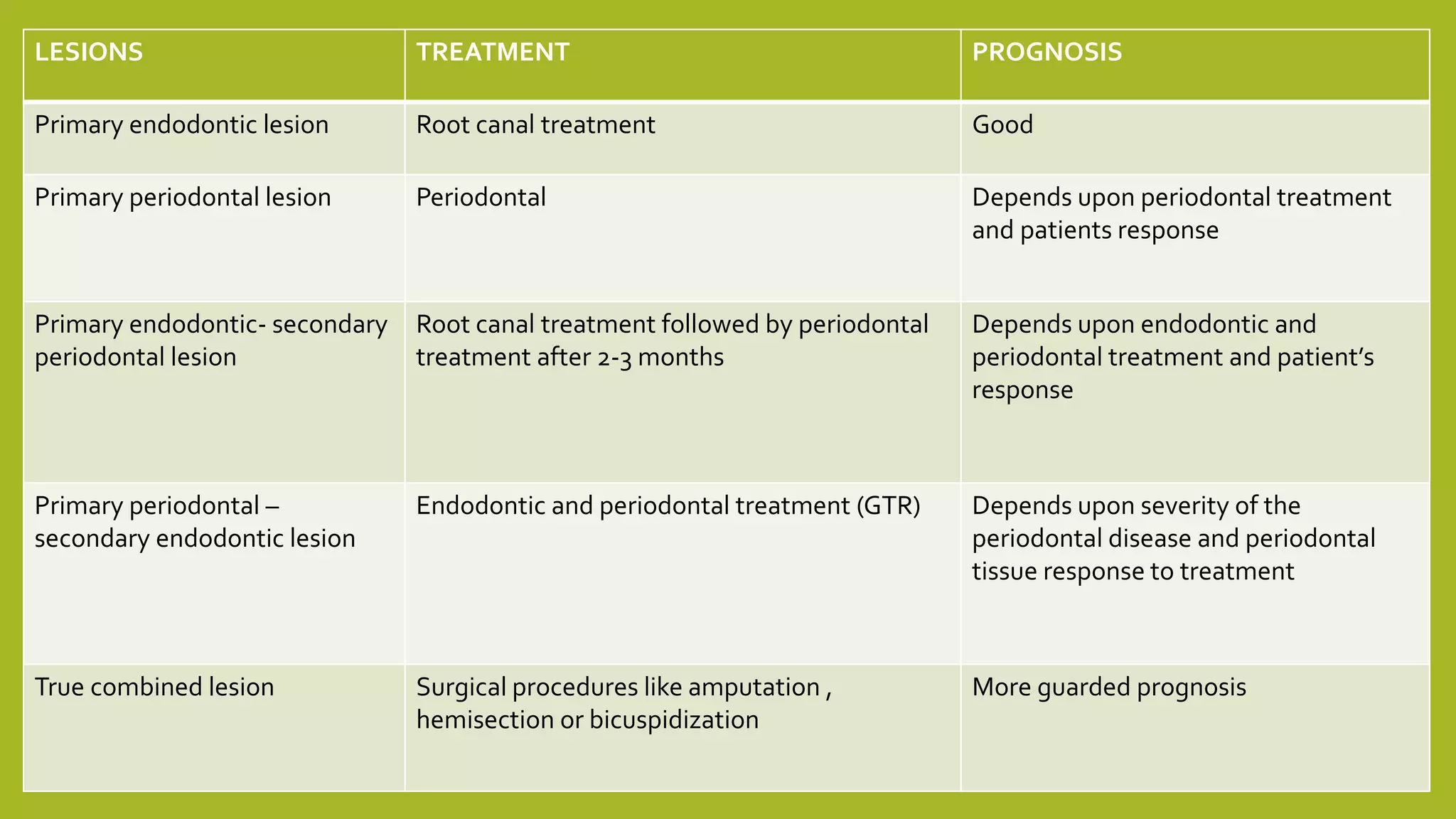
The document discusses endodontic-periodontal lesions, their pathways of infection, and classification systems for diagnosis. It covers Weine's and Simon, Glick, and Frank's classifications, emphasizing the differences between primary endodontic and periodontal lesions and their treatments. Treatment approaches, including surgical procedures and the prognosis for various lesion types, are also outlined.