Downloaded 645 times
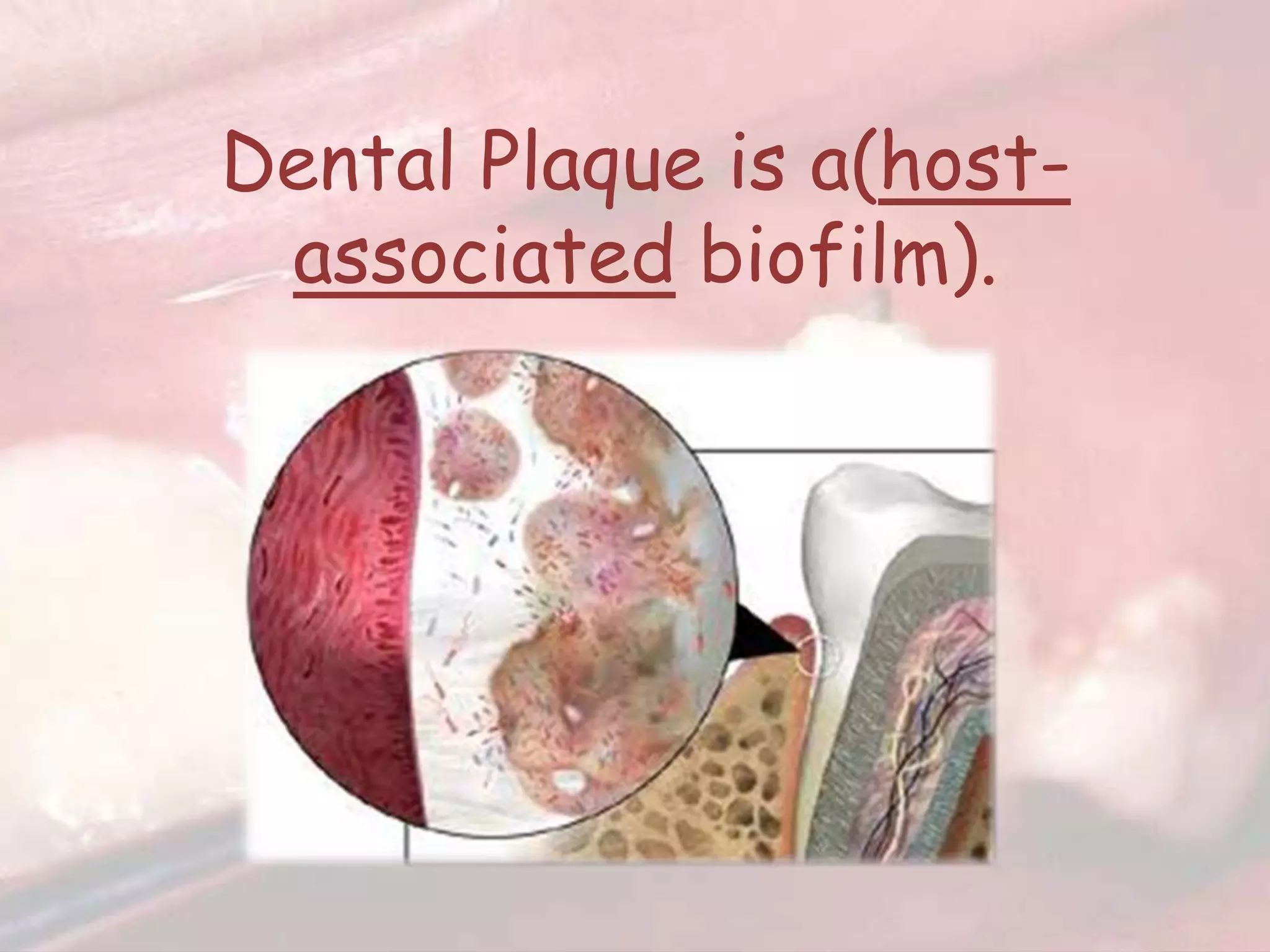
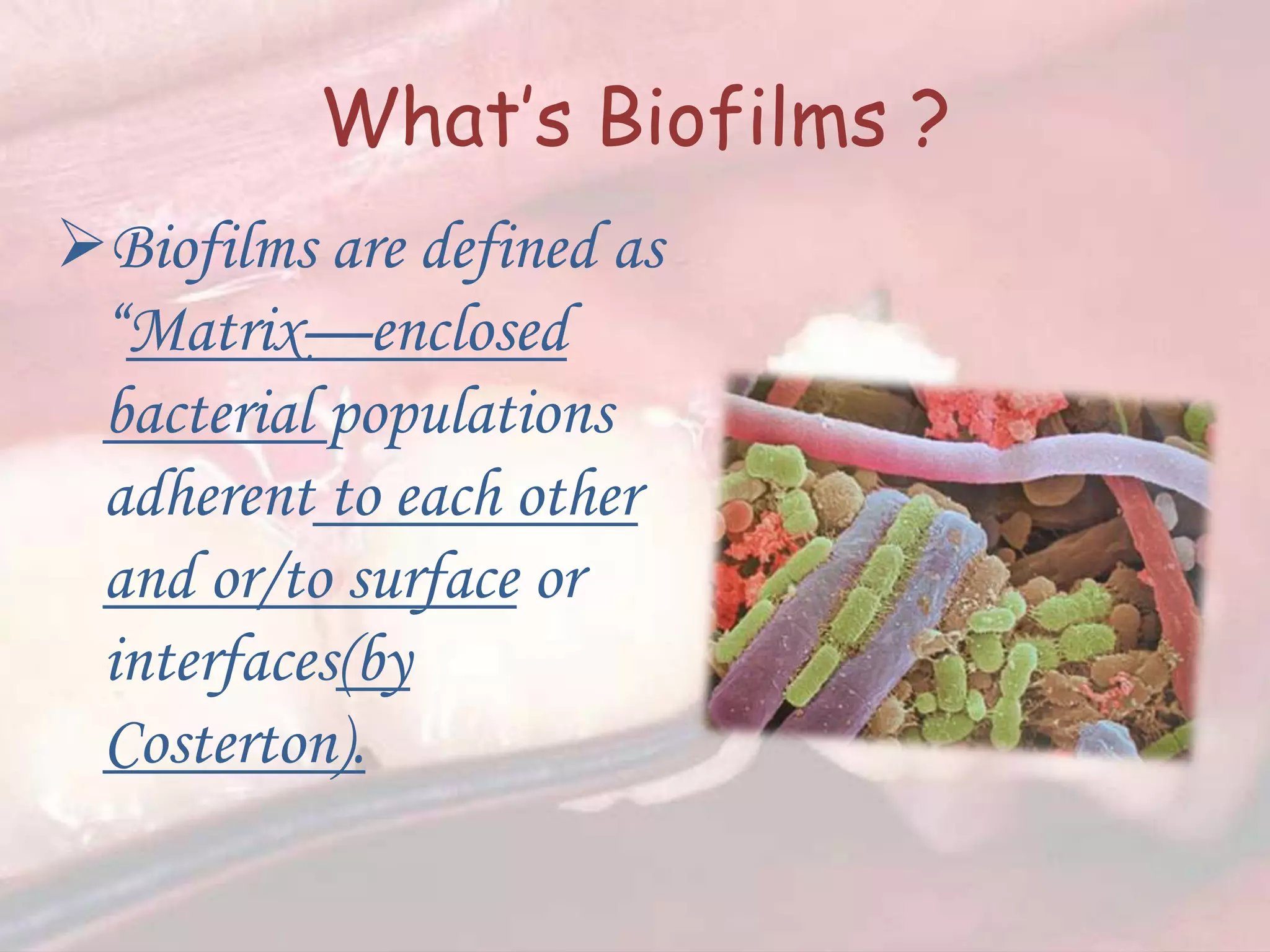



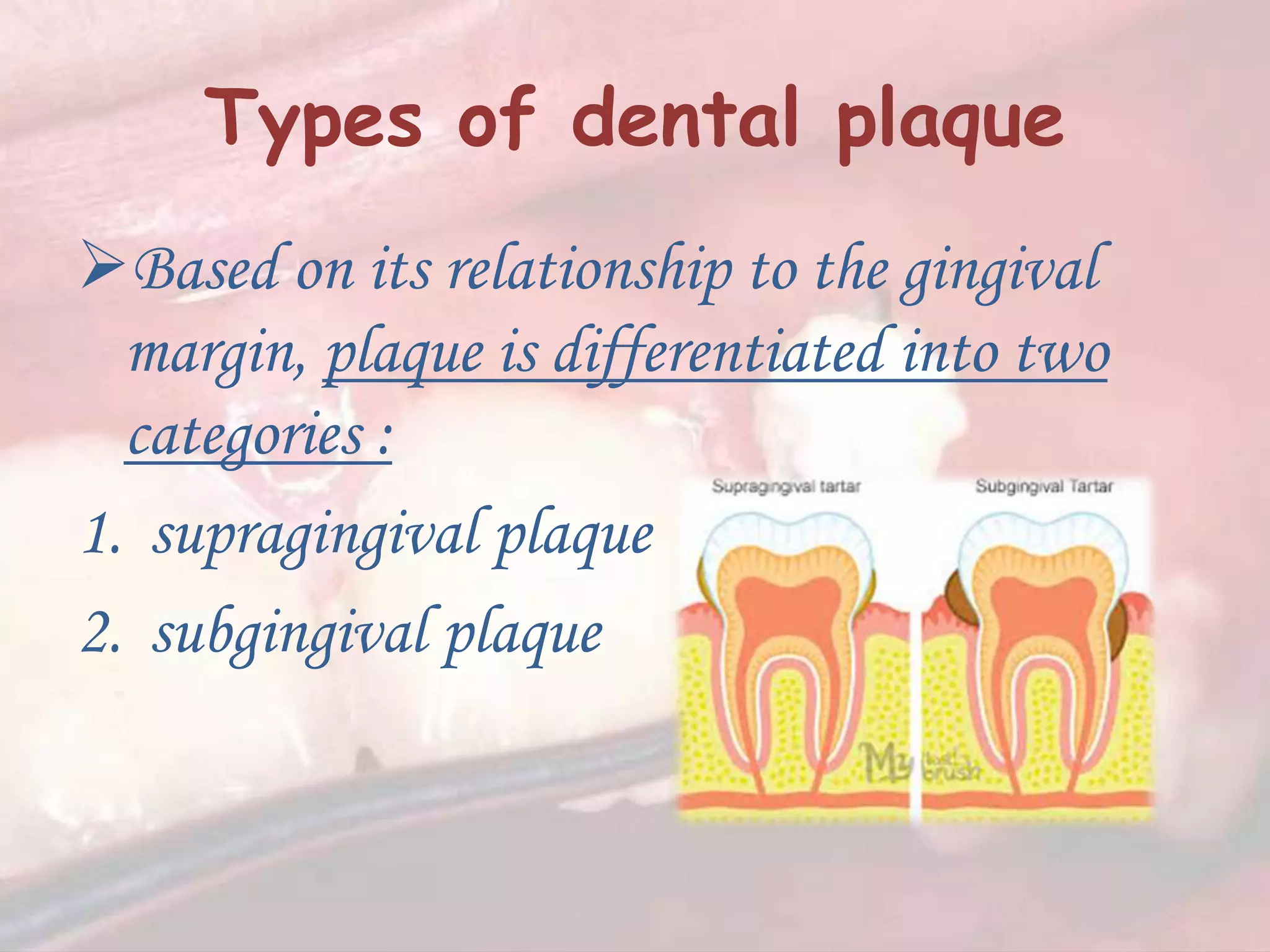
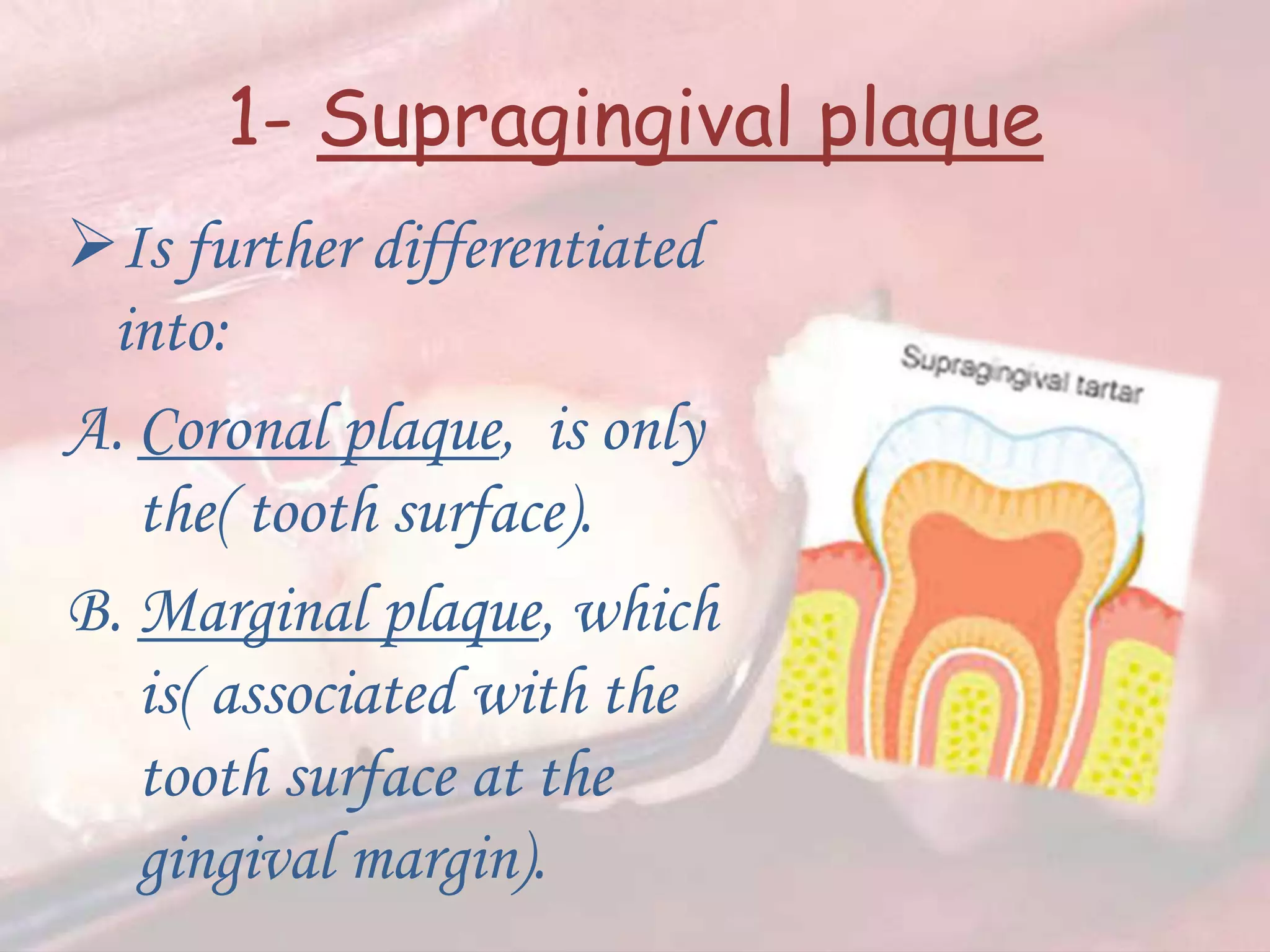

















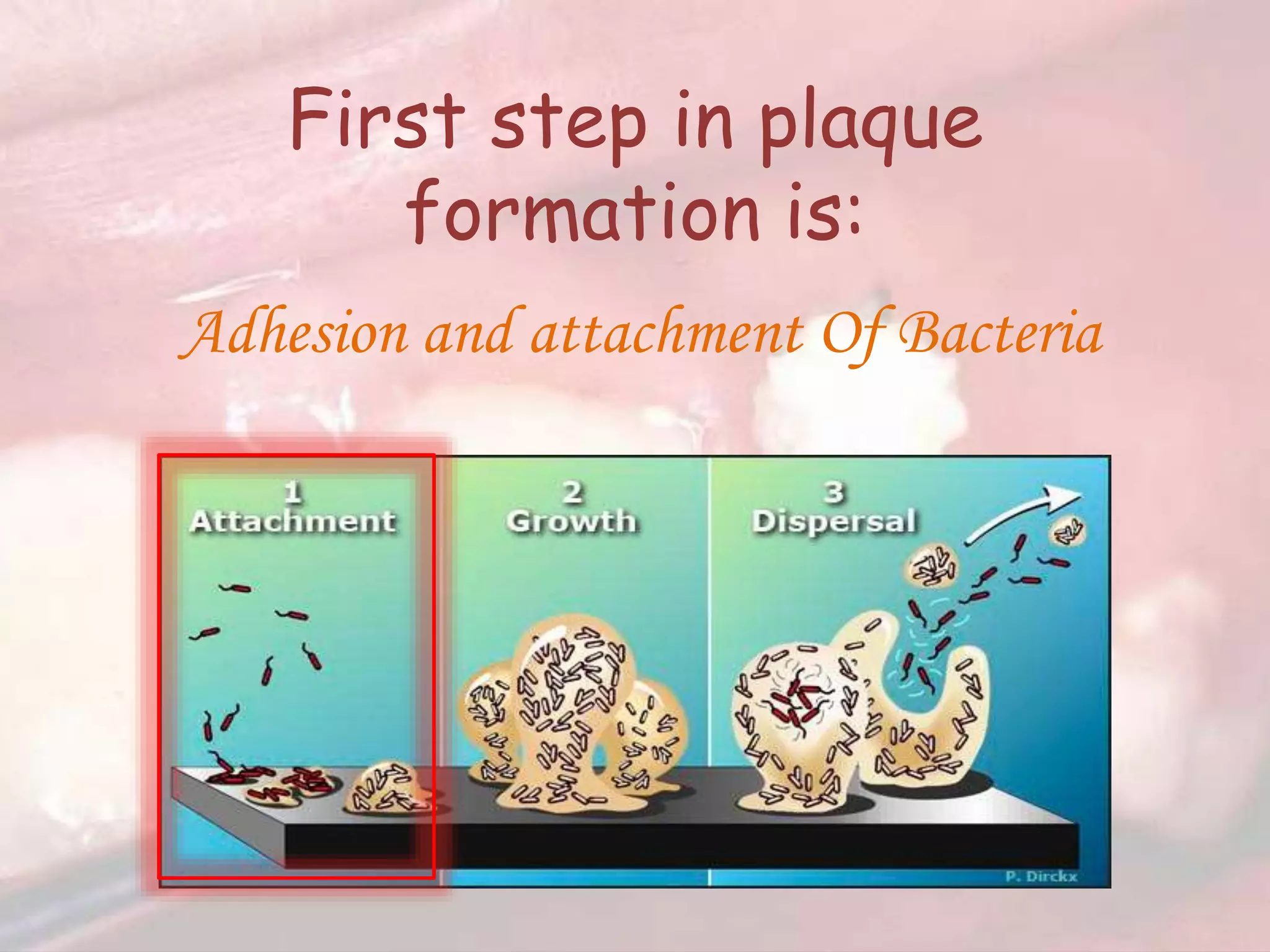






































Dental plaque is a biofilm composed of microorganisms adhering to tooth surfaces, which can be categorized into supragingival and subgingival plaque. The composition and pathogenicity of dental plaque vary, with specific bacteria associated with periodontal diseases, while its growth and accumulation depend on bacterial adhesion and interactions with the tooth surface. Understanding dental plaque's structure and microbial community is essential for the prevention and treatment of periodontal disease.













































































