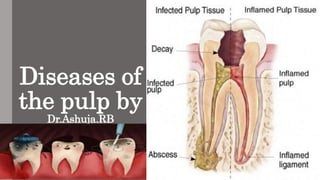
This document discusses diseases of the dental pulp. It begins with an introduction and definitions of key terms like pulp and pulpitis. It then covers the classification, causes, features, histopathology, treatment and prognosis of various pulp conditions like reversible and irreversible pulpitis, acute and chronic pulpitis, pulp polyps, and gangrenous necrosis. It distinguishes between the symptoms and characteristics of different types of pulpitis and pulp conditions. It provides an overview of diagnostic techniques and the typical pathway from normal pulp to pulp necrosis if left untreated.
In this presentation, it describes about the periapical diseases, for dental students.
very useful for endodontic purpose.
remember it does not include the pulpal diseases.
Apexogenesis & apexification in pediatric dentistryDr. Harsh Shah
SDDCH Parbhani
Presented by : Vipul GIratkar
Dept. of Pediatric dentitstry
Guided by . Dr. Rehan Khan
DIscussion regarding apexification and apexogenesis
Pericoronitis is inflammation of soft tissues surrounding the crown of partially erupted tooth including gingiva and dental follicle.
It can be acute, subacute or chronic.
The partially erupted or impacted mandibular third molar is the most common site of pericoronitis.
The lesion may be red swollen,suppurating along with the pain which may radiate to the surrounding tissues.
For more information book an appointment contact :
Dr.Rajat Sachdeva
Director & Mentor
Dr Sachdeva’s Dental Aesthetic And Implant Institute
I 101, Ashok Vihar Phase 1, Delhi- 110052
Contact us at
Phone : +919818894041,01142464041
Our Websites:
www.sachdevadentalcare.com
www.dentalimplantindia.co.in
www.dentalclinicindelhi.com
www.dentalcoursesdelhi.com
Google+ link: https://goo.gl/vqAmvr
Facebook link: https://goo.gl/tui98A
Youtube link: https://goo.gl/mk7jfm
Linkedin link: https://goo.gl/PrPgpB
Slideshare link : http://goo.gl/0HY6ep
Twitter Page : https://goo.gl/tohkcI
Instagram page : https://goo.gl/OOGVig
For Dentists : https://goo.gl/6t8DD5
In this presentation, it describes about the periapical diseases, for dental students.
very useful for endodontic purpose.
remember it does not include the pulpal diseases.
Apexogenesis & apexification in pediatric dentistryDr. Harsh Shah
SDDCH Parbhani
Presented by : Vipul GIratkar
Dept. of Pediatric dentitstry
Guided by . Dr. Rehan Khan
DIscussion regarding apexification and apexogenesis
Pericoronitis is inflammation of soft tissues surrounding the crown of partially erupted tooth including gingiva and dental follicle.
It can be acute, subacute or chronic.
The partially erupted or impacted mandibular third molar is the most common site of pericoronitis.
The lesion may be red swollen,suppurating along with the pain which may radiate to the surrounding tissues.
For more information book an appointment contact :
Dr.Rajat Sachdeva
Director & Mentor
Dr Sachdeva’s Dental Aesthetic And Implant Institute
I 101, Ashok Vihar Phase 1, Delhi- 110052
Contact us at
Phone : +919818894041,01142464041
Our Websites:
www.sachdevadentalcare.com
www.dentalimplantindia.co.in
www.dentalclinicindelhi.com
www.dentalcoursesdelhi.com
Google+ link: https://goo.gl/vqAmvr
Facebook link: https://goo.gl/tui98A
Youtube link: https://goo.gl/mk7jfm
Linkedin link: https://goo.gl/PrPgpB
Slideshare link : http://goo.gl/0HY6ep
Twitter Page : https://goo.gl/tohkcI
Instagram page : https://goo.gl/OOGVig
For Dentists : https://goo.gl/6t8DD5
Definition of pulpitis, Factors causing injury to the pulp, aerodontalgia, classification of pulpitis, clinical features of various types of pulpitis, histopathology and its treatment are inlisted in this presentation.
Endodontic emergencies and mid term flare upsDR POOJA
An endodontic emergency is defined as pain and/or swelling caused by inflammation or infection of pulp and/or periradicular tissue necessitating an emergency visit to the dentist for immediate treatment.
The main causative factors responsible for occurrence of endodontic emergencies are:
Pathosis in pulp and periradicular tissues
Traumatic injuries
Recent studies report a 60-82% incidence of endodontic emergencies among all dental emergencies.
Within this group, 20-42% of patients seek care for teeth with symptomatic irreversible pulpitis (SIP) .
Additionally, about 60% of SIP patients also complain of symptomatic apical periodontitis (SAP)
The goal of management of endodontic emergencies is to quickly and effectively manage pain and infections thereby also minimizing the development of persistent pain and the formation of periapical pathology.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
2. • Introduction
• Definition
• Classification
• Etiologic features
• Reversible and irreversible
• Acute pulpitis
• Chronic pulpitis
• Pulp polyp
• Gangrene of pulp
3. Introduction:
• Like other connective tissue pulp reacts with bacterial
infection or the other irritant by inflammatory response.
• Pulpitis is the most common lesion to produce.
• A focal breach in this barrier can adversely affect the
health of the dental pulp.
• Inflammatory vascular changes increase the pulpal
volume, but swelling is restricted due to the surrounding
dentinal walls, often triggering pain.
4. Definition:
Pulp:
Soft tissue within pulp cavity, consisting of connective t
issue containing blood vessels, nerves, and lymphatics,
and at the periphery, layer of odontoblasts capable of in
ternal deposition and repair of the dentin.
Periapical:
• Encompassing or surrounding the tip of the root of a
tooth.
Pulpitis :
• Inflammation of the pulp of a tooth.
5. Clinically normal pulp
• Clinically, a normal pulp exhibits no signs or symptoms
that suggest pulpitis.
• Teeth respond to cold with mild pain that resolves in 1 to
2 seconds, whereas heat is not associated with pulpal
discomfort.
• No pain on percussion.
• Radiographic examination of the periradicular bone will
be within normal limits.
6. History
• During World War II in flying personnel,condition
clinically simulating pulpitis by the incidence of
toothache was reported - aerodontalgia.
• Described in aircrew flying at high altitudes, astronauts,
submarine crews, and in deep sea divers.
• It is relatively uncommon and is associated particularly
with recently filled teeth.
7. • The pain in decompression does not usually occur in normal
pulps.
• Some cases of pain localized to the dental area and resembling
aerodontalgia have been reported to represent aerosinusitis
and not to be related to the teeth.
8. Classification:
1. Depending on severity:
• Acute and chronic
2. Depending upon the extent of involvement of pulp
• Partial or focal pulpitis
• Total pulpitis or generalized pulpitis
3. Based on the communication between pulp and oral environment
• Open pulpitis (Pulpitis Aperta)
• Closed pulpitis (Pulpitis Clausa)
9. Etiologic features:
• Four main types of noxious stimuli are common
causes of pulpal inflammation (pulpitis):
1.Mechanical damage:
Traumatic accidents, iatrogenic damage from dental procedures,
attrition, abrasion, and barometric changes.
2. Thermal injury: Cavity preparation, polishing, and exothermic
chemical reactions of dental materials.
10. 3. Chemical irritation:
Erosion or from the inappropriate use of acidic dental materials.
4. Bacterial effects:
Bacteria can damage the pulp through toxins or directly after
extension from caries or transportation via the vasculature.
11. • Anachoretic pulpitis: Bacteria circulating in the blood stream
tend to settle out or accumulate at sites of pulpal inflammation,
such as that which might follow some chemical or mechanical
injury to the pulp.
• Anachoresis is a phenomenon by which blood borne bacteria,
dyes, pigments, metallic substances, foreign proteins, and other
materials are attracted to the site of inflammation.
12. • Cause: Increased capillary permeability in
the particular area.
• Anachoretic pulpitis probably occurs in a
clinically irrelevant number compared
with the number of cases occurring as a
result of dental caries.
13. Cracked tooth syndrome
• In cracked tooth syndrome, a tooth, usually a restored premolar
may split under masticatory stress.
• These cracks are often minute and invisible clinically, and they
allow the bacteria to enter into the pulp.
14. • Bacterial invasion may also occur as a result of a
bacteremia and septicemia.
• Pulpitis may rarely follow chronic periodontal disease
wherein the microorganisms enter through the accessory
canals of the exposed root surface especially through
lateral canals infurcation areas of molars.
15. Reversible pulpitis
• One of the earliest forms of pulpitis - focal
reversible pulpitis.
• Pulp hyperemia.
• vascular dilatation can occur artefactually from
the ‘pumping’ action during tooth extraction as
well as pathologically as a result of dentinal and
pulpal irritation.
• Therefore, this early mild transient pulpitis,
localized chiefly to the pulpal ends of irritated
dentinal tubules, is now known as focal reversible
pulpitis.
16. Clinical Features:
• A tooth is sensitive to cold.
• The application of ice or cold fluids pain.
• Pain disappears upon removal of the thermal stimuli or
restoration of the normal temperature.
• Tooth responds to stimulation by the electric pulp tester at a
lower level of current.
• Deep carious lesion, large metallic restorations,or ,
restorations with defective margins.
17. Histologic Features:
• Dilatation of the pulp vessels
• Edema fluid may collect
• Allowing actual extravasation of red blood cells or some
diapedesis of white blood cells.
• Thrombosis.
18. Treatment and Prognosis.
• Reversible condition
• The irritant is removed before the pulp is severely
damaged.
• Excavation of caries and restoration or a replacement of
defective filling
• If the primary cause is not corrected, extensive pulpitis
subsequent ‘death’ of the pulp.
19. Irreversible pulpitis
• Patients with early irreversible pulpitis generally have
o sharp, severe pain on thermal stimulation,
o pain continues for a longer period of time after the
stimulus is removed.
• Cold is especially uncomfortable,
• Even heat or sweet and acidic foods also can elicit pain.
20. • Early stages
o The pain often easily localized.
o With increasing discomfort,unable to identify the offending
tooth within a quadrant.
o Although pulpal pain never crosses the midline,it can be
referred from arch to arch,
o In difficult cases, pulp testing of both arches.
21. • Late stages
o The pain increases in intensity
oAs a throbbing pressure that can keep patients awake at
night.
o At this point, heat increases the pain; however, cold may
produce relief.
oElectric pulp testing - at higher levels of current or
demonstrates no response.
o Mobility and sensitivity to percussion are usually absent.
oIf pulpal drainage occurs ,symptoms may resolve if the
22. Histological features:
• The dental pulp exhibits an area of
fibrosis and chronic inflammation
peripheral to the zone of abscess
formation.
Irreversible Pulpitis. Dental pulp
exhibiting acute inflammatory infiltrate
consisting predominantly of
polymorphonuclearleukocytes.
23. Treatment:
• Complete removal of pulp or pulpectomy
• Placement of intracanal medicament
• Extraction or root canal therapy
24. Features of reversible and irreversible pulpitis
Reversible pulpitis Irreversible pulpitis
Pain in short, sharp stabs Constant throbbing pain with sharp
exacerbations
Stimulated by cold as hot and cold or osmotic (sweet)
stimuli.
In late stages cold may relieve the
pain
Pain resolves after
stimulus removed in
seconds or a few minutes<
20 minutes duration
Pain persists several minutes or
hours after an exacerbating
stimulus> 20 minutes duration
Easily localized Difficult to localize
Unaffected by position Affected by position
25. Acute pulpitis
• Extensive acute inflammation of the dental
pulp.
• Frequent immediate sequela of focal reversible
pulpitis.
• It may also occur as an acute exacerbation of a
chronic inflammatory process.
26. Causes:
• Large carious lesion or restoration,
• ‘Recurrent caries’.
Clinical features:
• Early stages
o Involves only a portion of the pulp(beneath the carious
lesion)
o Severe pain is elicited by thermal changes, particularly to
ice or cold drinks.
o Pulpal pain is poorly localized.
o Pain persists even after the thermal stimulus has
disappeared or been removed.
27. Late stage:
• The pain may become even more severe.
• Pain - lancinating or throbbing type.
• The pain generally lasts for 10–15 minutes but may be
more or less continuous.
• Teeth of the upper or lower jaw of the affected side.
• Its intensity may be increased when the patient lies
down.
• The application of heat may cause an acute exacerbation
of pain.
28. • The electric pulp vitality tester - lower level of current
than adjacent normal teeth, indicating increased
sensitivity of the pulp.
• When necrosis of the pulp tissue occurs, this sensitivity is
lost.
• Severe pain - entrance to the diseased pulp is not wide
open.
• Severe acute pulpitis is extremely uncomfortable and at
least mildly ill.
29. Histopathologic features:
• Early acute pulpitis is characterized by the
o Continued vascular dilatation seen in focal reversible
pulpitis,
oAccumulation of edema fluid in the connective tissue
surrounding the tiny blood vessels.
o Increased PML becomes apparent along the walls of
these vascular channels,
o leukocytes rapidly migrate through the endothelium
lined structures.
30. • WBC are found in the inflamed region, beneath an
area of carious penetration, the odontoblasts usually
destroyed in this area.
• The entire odontoblastic layer degenerates.
• Entire pulp tissue undergoes rather rapid
disintegration ,when there is closed pulp.
• Numerous small abscesses may form.
31. • Eventually the entire pulp undergoes liquefaction
and necrosis.
• Acute suppurative pulpitis.
• The pulp, especially in the later stages of pulpitis
following carious invasion, contains large
numbers of bacteria.
33. Chronic pulpitis
• May arise on occasion through quiescence of a previous
acute pulpitis.
• But more frequently it occurs as the chronic type of
disease from the onset.
• The signs and symptoms are considerably milder than
those in the acute form of the disease.
34. Clinical Features:
• Pain
o Not a prominent feature.
o Even sometimes the patient complains of a mild, dull ache.
o More often intermittent than continuous.
• The reaction to thermal change is dramatically reduced in
comparison to that in acute pulpitis.
• The general features are not typical.
• In the absence of significant symptoms, serious involvement
of the pulp may be present.
35. • Even in wide-open carious lesions with open pulp, there
is relatively little pain.
• Bleeding may occur, pain is often absent.
• Pulps may become totally necrotic without pain.
36. Histologic Features:
• Chronic pulpitis is characterized by infiltration of the
pulp tissue by varying numbers of mononuclear cells,
chiefly lymphocytes and plasma cells and more vigorous
connective tissue reaction.
• Capillaries are usually prominent;
• Fibroblastic activity is evident;
• Collagen fibers arranged in bundles.
37. • Sometimes the pulp attempt to ward off the infection
through deposition of collagen fibers around the inflamed
area.
• The tissue reaction may resemble the formation of
granulation tissue on the surface of the pulp tissue in a wide-
open exposure.
38. • With bacterial stains,microorganisms may be found in the
pulp tissue, especially in the area of a carious exposure.
• In some cases, the pulpal reaction fluctuates between an
acute and a chronic phase.
39. Treatment and Prognosis:
• Does not differ intensely from that of acute pulpitis.
• Root canal therapy or extraction of the tooth.
40. Pulp polyp
• Chronic hyperplastic pulpitis
• A unique form of pulpitis
• The inflamed pulp, instead of perishing by continued
suppuration, reacts by excessive and exuberant
proliferation.
• It occurs either as a chronic lesion from the onset or
as a chronic stage of a previously acute pulpitis.
41. Clinical features :
• Children and young adults.
• It involves teeth with large, open carious lesions.
• Appears as a pinkish-red globule of tissue protruding from
the pulp chamber.
42. • Deciduous molars and the first permanent molars.
• Have an excellent blood supply.
• Unusual proliferative property of the pulp tissue.
• Tooth is asymptomatic except for a possible feeling of
pressure when it is placed into masticatory function.
43. Histopathological features:
• The surface may or may not be covered with
stratified squamous epithelium, which migrates
from the adjacent gingiva or arises from sloughed
epithelium within the oral fluids.
• The deeper pulp tissue within the canals
typically shows fibrosis and a chronic
inflammatory infiltrate.
• Pulpal calcifications are common in both the
radicular and coronal portions.
44. • Often the apical portion of the pulp tissue is normal with
minimal inflammation or fibrosis.
• The well-vascularized granulation tissue mass often
becomes epithelialized, presumably by auto
transplantation of epithelial cells from nearby mucosal
surfaces.
46. Gangrenous necrosis of pulp
• Untreated pulpitis, either acute or chronic complete
necrosis of the pulp tissue.
• Generally associated with bacterial infection, the term pulp
gangrene has sometimes been applied to this condition.
• Gangrene being defined as necrosis of tissue with
superimposed bacterial infection.
47. • Cause: sudden traumatic event, untreated irreversible
pulpitis.
• Infected pulpal necrosis: Dental decay Pain
• Non infected pulp necrosis: No symptoms for many months.
48. • First sign in non infected : Discoloration of tooth due to
result of the decomposing tissue debris and breakdown
products of RBCs entering the open ends of the dentinal
tubules and becoming distributed throughout the dentin.
• After tooth is non vital - Tooth loses its ability to
rehydrate the dentin, making it more brittle and subject
to cracks and fracture.
49. • Associated with a foul odor
• Diagnostic tool to determine pulpal necrosis – Percussion test
• Gently tapping on several teeth in the area with a blunt instrument
because pressure from tapping will produce intense pain.by this its
easily identified if tooth has undergone pulpal necrosis.
50. • Necrosis of pulp has been reported in sickle cell anemia where
there is blockage of pulp microcirculation by sickle
erythrocytes .
• Dry gangrene sometimes occurs when the pulp dies for some
unexplained reason.
• The nonvital pulp maintains its general histologic
characteristics, being non purulent.
• This condition may be due to some traumatic injury or infarct.
51. • Pulp gangrene should not be considered a specific form of
pulp disease but simply the most complete end result of
pulpitis in which there is total necrosis of tissue.
• following blockage of the pulp microcirculation by sickled
erythrocytes.
• Associated with a foul odor when such infected pulps are
opened for endodontic treatment.
• Necrosis of pulp has been reported in sickle cell anemia
where there is blockage of pulp microcirculation by sickle
erythrocytes
52. Key features of pulpitis
• Caused by infection or irritation of the pulp, usually by caries.
• Severe stabbing pain in a tooth, triggered by hot or cold food or
starting spontaneously, indicates acute irreversible pulpitis.
• Pulp pain is poorly localized
• Chronic pulpitis is often symptomless.
• Untreated pulpitis usually leads to death of the pulp and
spread of infection to the periapical tissues.
53. Treatment options for pulpitis:
• If fractured or cracked, stabilise fracture and seal pulp
temporarily.
• Removal of caries, obtundent or steroid dressing
• Removal of caries and pulp capping
• Pulpotomy in deciduous teeth
• Endodontic treatment
• Extraction
• Analgesics are largely ineffective.
55. Diagnostic techniques
• History and nature of the pain
• Reaction to thermal changes
• Reaction to mild electric stimulation
• Reaction to percussion of tooth
• Radiograph examination
• Visual examination
• Palpation of surrounding area
56. Guess the diagnosis?
1.
• Sharp intense pain
• Pain is spontaneous
• Sensitive to cold
• Pain remains for 5 to 10 minutes.
• Low level current responding by patient on electric pulp
testing.
• Pain disappears on removal of thermal irritant
58. 2.
• Dull pain
• Frequent pain
• Sensitive to hot
• Pain keeps patient awake at night on lying down to sleep
• Difficult to localize the tooth.
• Responds to higher level current on electric pulp testing
• On removal of stimuli,pain lingers for longer time.
60. 3.
• Patient may complain of growth of tissue on tooth
• Painless
• Discomfort while chewing
• Children and young adults
• Deciduous molars + 1st permanent molar
• Clinically, open carious lesion and red globe like tissue
protruding from tooth.
Pulpitis, if untreated, is often followed by death of the pulp and spread of infection through the apical foramen into the periapical tissues to cause periapical periodontitis.
This pain has been attributed to the formation of nitrogen bubbles in the pulp tissue or vessels.
Mechanical sources of injury include traumatic accidents, iatrogenic damage from dental procedures, attrition, abrasion, and barometric changes.
Severe thermal stimuli can be transmitted through large uninsulated metallic restorations or may occur from such dental procedures as cavity preparation, polishing, and exothermic chemical reactions of dental materials.
The pathways by which microorganisms may invade the pulp and periapical tissues: (1) from the apical foramen, (2) via the periodontal ligament and (3) via the blood stream (anachoresis).
The significance of microorganisms in the etiology of pulpitis has been confirmed who produced surgical pulp exposures in germ-free rats. It
was found that no devitalized pulps or periapical infections developed even when gross food impactions existed. By contrast, conventional animals rapidly developed complete pulpal necrosis.
One of the earliest forms of pulpitis is the condition known as focal reversible pulpitis.
Teeth in which this condition exists usually show deep carious lesion large metallic restorations (particularly without adequate insulation), or restorations with defective margins.
It will be found also that such a tooth responds to stimulation by the electric pulp tester at a lower level of current, indicating a lower pain threshold (or a greater sensitivity) than that of adjacent normal teeth.
Focal pulpitis is characterized microscopically
Reversible Pulpitis. Dental pulp exhibiting hyperemia and edema. Edema fluid may collect because
of damage to the capillary walls.
The adjacent dentin was cut recently during placement of a dental restoration.
Slowing of the blood flow and hemoconcentration due to
transudation of fluid from the vessels conceivably could cause thrombosis.
Mobility and sensitivity to percussion are usually absent because significant inflammation has not spread yet to the apical area.
If pulpal drainage occurs (e.g., crown fracture, fistula formation), then the symptoms may resolve—only to return if the drainage ceases.
Irreversible Pulpitis. Dental pulp exhibiting acute inflammatory infiltrate consisting predominantly of polymorphonuclearleukocytes.
Irreversible Pulpitis. Same tooth as depicted in above pic. The dental pulp exhibits an area of fibrosis and chronic inflammation peripheral to the zone of abscess formation.
Even in its early stages when the inflammatory reaction involves only a portion of the pulp, usually in the area just beneath the carious lesion, relatively severe pain is elicited by thermal changes, particularly when taking ice or cold drinks.
and may be felt in any
of the teeth of the upper or lower jaw of the affected side,.
accumulation of edema fluid in the connective tissue surrounding the tiny blood vessels.
The reaction to thermal change is dramatically reduced in comparison to that in acute pulpitis. Because of the degeneration of nerve tissue in the affected pulp, the threshold for stimulation by the electric pulp vitality tester is often increased.
Bacterial products may act as antigens and the dendritic cells of the pulp capture the antigens, migrate to lymph nodes and present them to lymphocytes.
These activated T cells then leave the lymphnodes and reach the pulp.
Children and young adults who respond to proliferative lesions.
Have an excellent blood supply because of the large root opening.
The open chronic pulpitis an ample blood supply and the increased regenerative capacity of young pulpal tissue appears in some instances to stimulate the pulpal tissue to proliferate or to produce granulation tissue.
The surface of the polyp may or may not be covered with stratified squamous epithelium, which migrates from the adjacent gingiva or arises from sloughed epithelium within the oral fluids.
Since this is generally associated with bacterial infection, the term pulp gangrene has sometimes been applied to this condition,
Discolor is due to result of the decomposing tissue debris and breakdown products of RBCs entering the open ends of the dentinal tubules and becoming distributed throughout the dentin.
Tooth loses its ability to rehydrate the dentin, making it more brittle and subject to cracks and fracture.
Gently tapping on several teeth in the area with a blunt instrument because pressure from tapping will produce intense pain.by this its easily identified if tooth has undergone pulpal necrosis.
Pulp gangrene should not be considered a specific form of pulp disease but simply the most complete end result of pulpitis in which there is total necrosis of tissue.
following blockage of the pulp microcirculation by sickled erythrocytes.
Associated with a foul odor when such infected pulps are opened for endodontic treatment.
Necrosis of pulp has been reported in sickle cell anemia where there is blockage of pulp microcirculation by sickle erythrocytes
Nature n history: Duration n type of sensation, circumstances of its occurrences.
Reversible – sharp, intense pain
irreversible pain: dull,frequently vague in its location.
Reaction to thermal changes: hot or cold
Reversible: Immediate, sharp pain last for upto 20 mins
Irreversible : dull pain lasts for much longer duration.
Reaction to mild electric stimulation:
Reversible : nerves will be easily excited so respond to lower than normal voltage level.
Irreversible: nerve tissue within pulp is more severely damaged so higher level of voltage is required before the patient responds.
Reaction to percussion of tooth:
Positive reaction indicates inflammation in the apical periodontal tissue of a particular teeth in irreversible pulpitis
Radiograph examination:
Indicates irreversible changes within pulp.
Determine the cause of vague pain in a quadrant of the mandible or maxilla.
Visual examination:
Reveal any expansion of cortical plates of alveolar bone.small nodule over the apex of thetooth represent opening of a draining sinus tract of apical abscess.
Palpation of surrounding area
Pain in patient signifies that inflammation has reached the tissue surrounding the apex of the tooth.
Pulp is necrotic so pulp chamber need to be filled to prevent further spreading of inflammation to the surrounding bone.