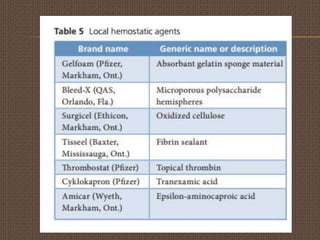
1) Dental care for patients with bleeding disorders has improved with new materials, hemostatic agents, preventative techniques, and minimally invasive procedures.
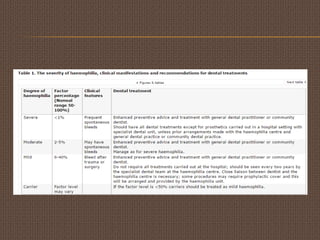
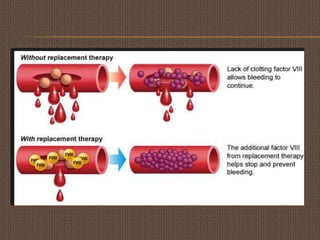
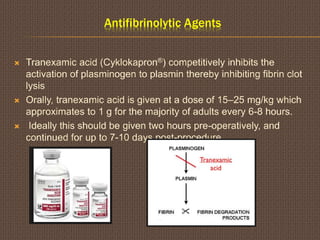
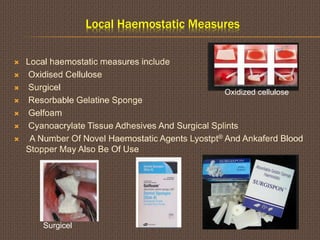
2) There are several types of bleeding disorders including hemophilia A/B and von Willebrand disease. Management strategies depend on the specific disorder and may include factor replacement therapy, desmopressin, antifibrinolytic drugs, or local hemostatic measures.
3) Dental procedures carry varying risks for patients with bleeding disorders depending on the need for local anesthesia or other invasive techniques. Proper treatment planning and hemostatic protocols are necessary to safely provide dental care.




![Desmopressin (Desamino-8-d-arginine Vasopressin [DDAVP])
The synthetic antidiuretic hormone, desmopressin, stimulates
release of endogenous FVIII and vWF from stores in patients with
mild haemophilia and Vwd
DDAVP can be administered one hour pre-procedure
subcutaneously (0.3 μg/kg using the 15 μg/ml concentration)
.Alternatively, DDAVP (0.3 μg/kg in 50 ml of normal saline) can be
administered intravenously (4 μg/ml concentration) one hour pre-
procedure as a slow intravenous infusion over 20–30 minutes.
Fluid intake should be restricted for around 24 hours after DDAVP
is given.](https://image.slidesharecdn.com/haemophilia-150709090153-lva1-app6891/85/Haemophilia-14-320.jpg)

























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)