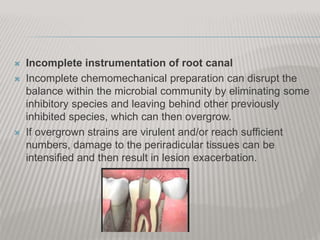
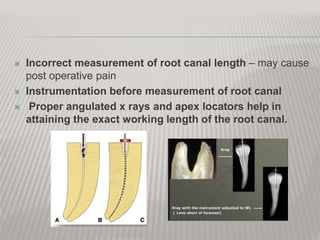
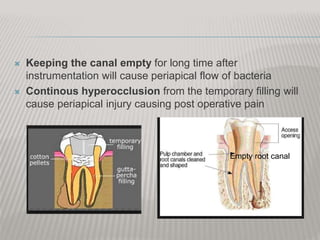
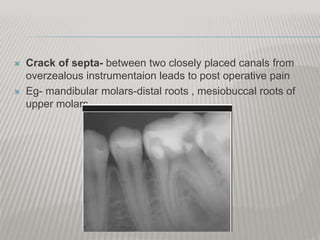
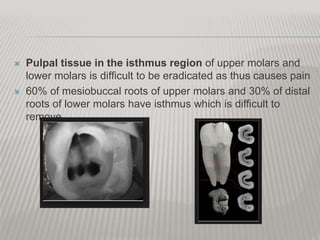
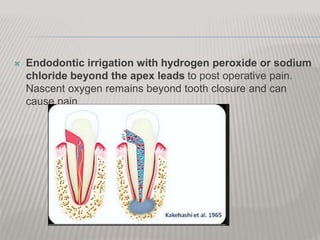
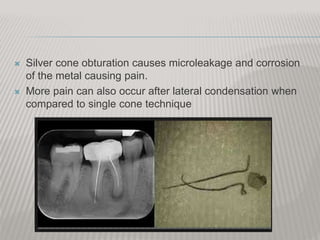
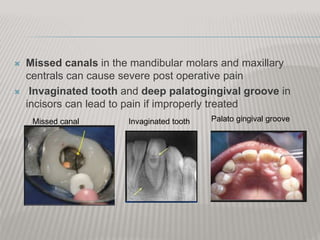
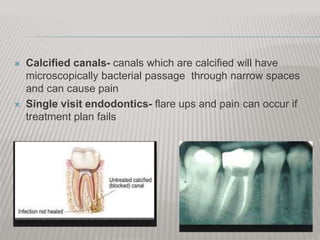
This document discusses factors that can cause pain during and after endodontic treatment. Mechanical, chemical, or microbial injury to the pulp or surrounding tissues during treatment can trigger an inflammatory response and pain. Specifically, vigorous instrumentation beyond the root apex, incomplete cleaning and shaping of the root canal leaving behind bacteria, extrusion of debris into tissues, and leaving the canal open too long after treatment can all cause pain. Ensuring proper working length, thorough cleaning and disinfection of canals, and temporary fillings that don't cause hyperocclusion can help prevent post-operative pain.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


