Downloaded 395 times

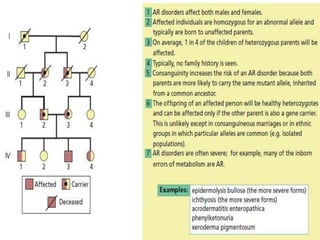
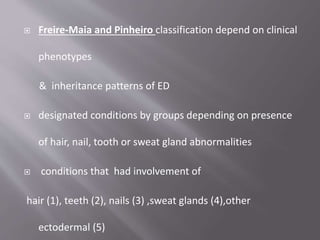




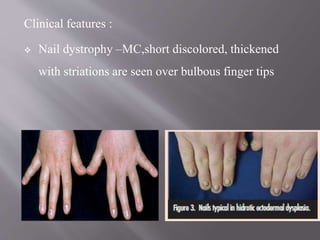
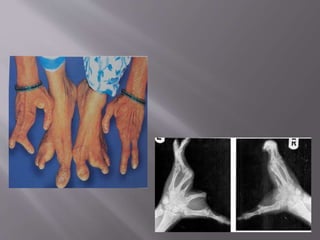



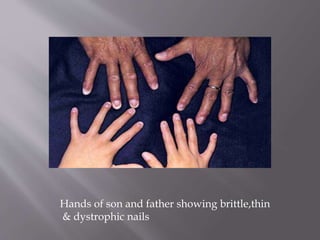
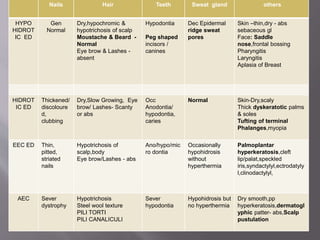
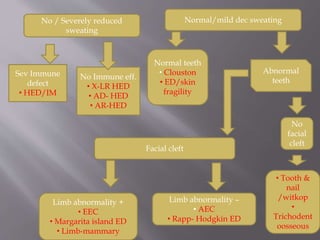


Ectodermal dysplasias (EDs) are a group of inherited disorders that affect two or more ectodermal structures such as hair, teeth, nails, and sweat glands. They are caused by genetic defects that may be inherited or occur spontaneously. EDs are classified based on clinical phenotypes and affected structures. The most common types are hypohidrotic ED (affecting hair, teeth, nails and sweat glands) and hidrotic ED (affecting hair, teeth, and nails). Without proper care, ED patients can experience life-threatening hyperthermia, infections, and failure to thrive. Treatment focuses on managing symptoms and may involve dentures, skin care, eye protection, and environmental thermal
































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







