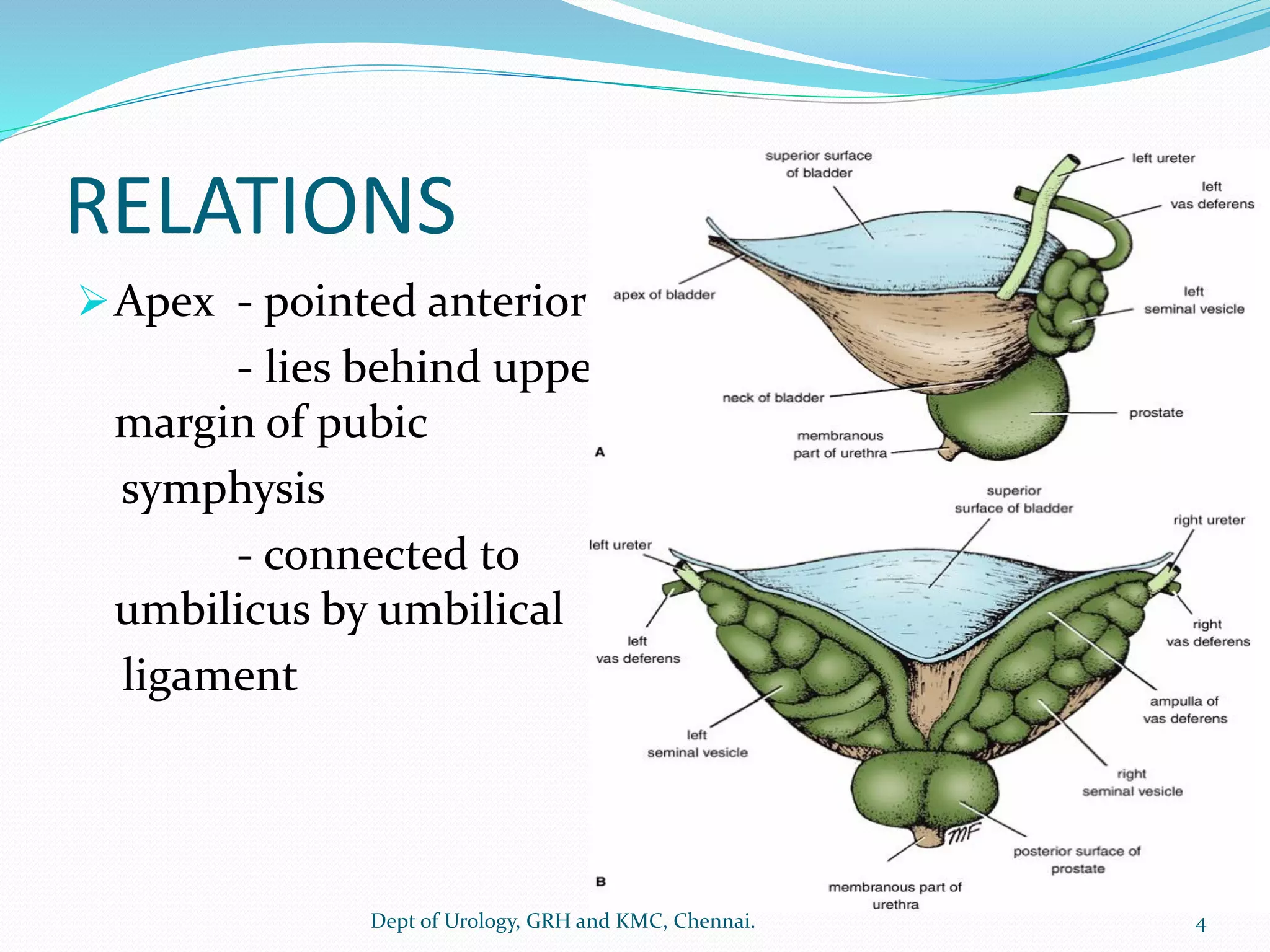
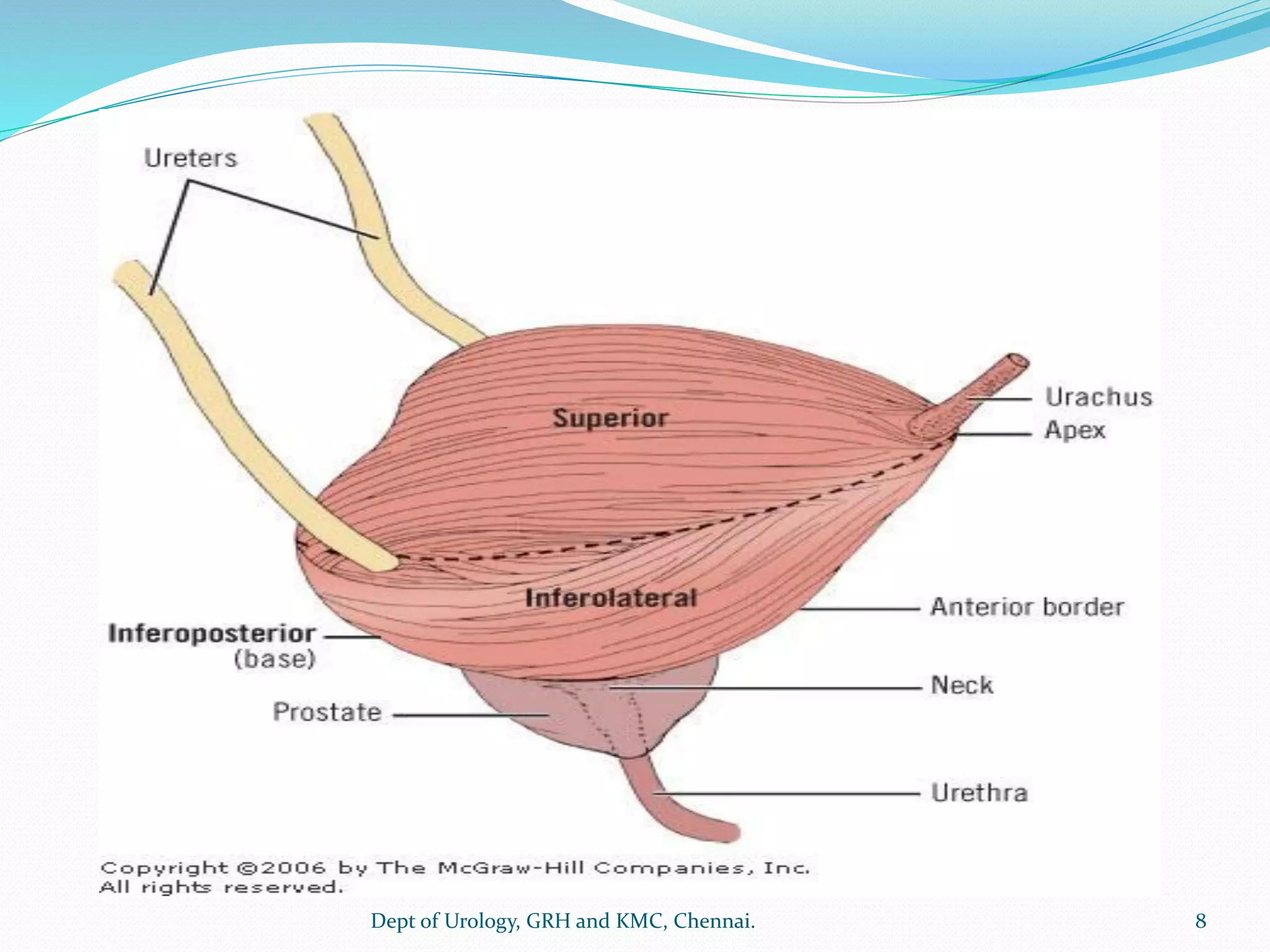
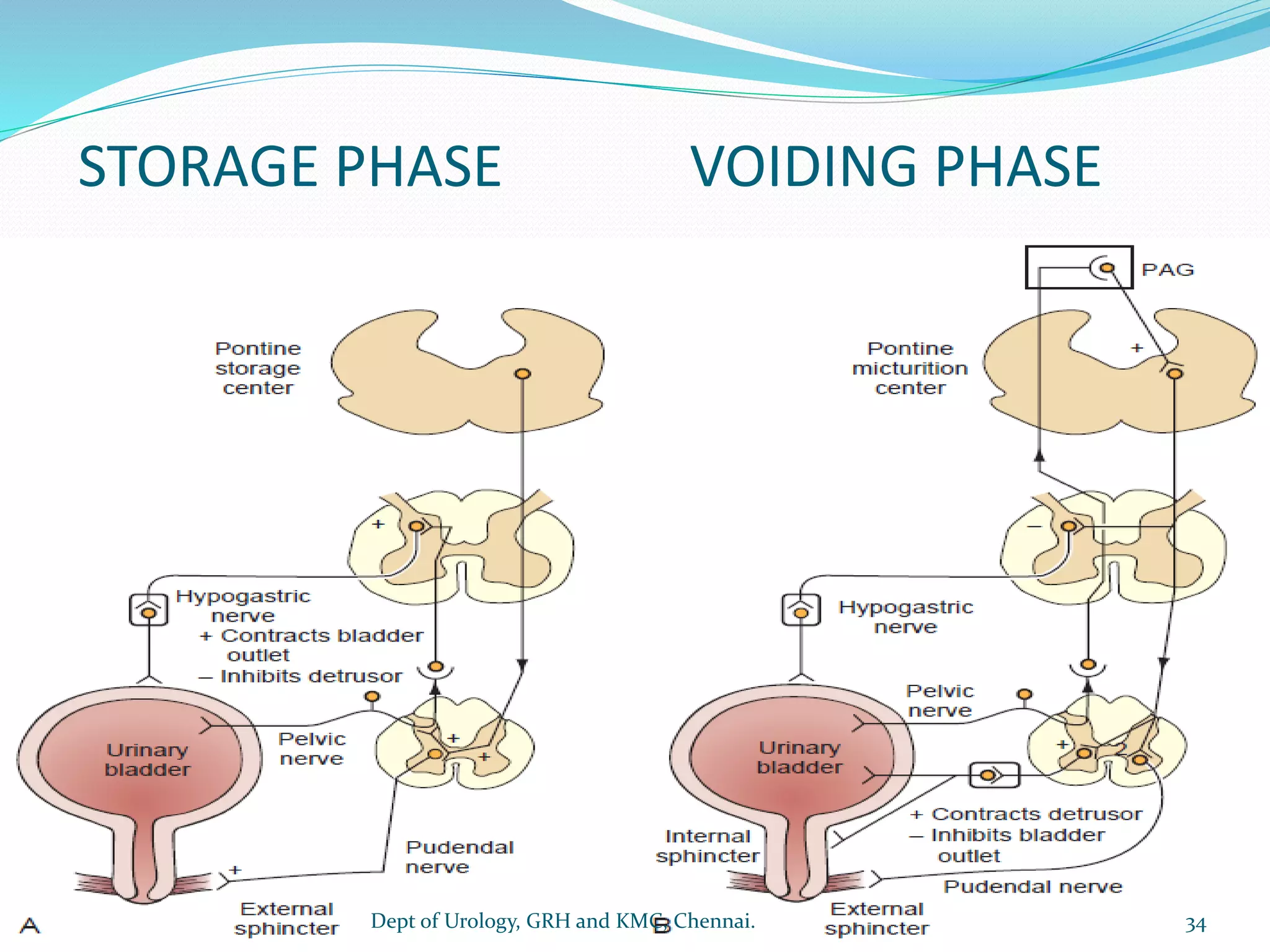
This document provides an overview of the anatomy and physiology of the urinary bladder. It describes the bladder's location, shape, relations to surrounding structures, blood supply, innervation, and histological layers. Key points include that the bladder is a hollow, retroperitoneal organ located in the pelvis that stores and empties urine. It has multiple ligaments attaching it to surrounding structures. The document also summarizes the normal filling and voiding functions of the lower urinary tract and the roles of the detrusor muscle, urethral sphincter, and neural control.