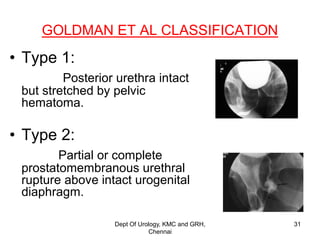
This document discusses the anatomy of the urogenital triangle and classification of urethral injuries. It begins with an overview of the bony pelvis and ligaments, followed by the muscles that support the pelvic floor including the levator ani and coccygeus. It then describes the urogenital diaphragm and its contents. Several classifications of urethral injuries are presented, including the McCallum & Col Pinto classification for posterior injuries and the AAST classification system for severity grading. Injuries can be anterior or posterior, with posterior injuries often associated with pelvic fractures from trauma.












































































![ANATOMY OF THE LOWER URINARY TRACT AND MALE [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anatomyofthelowerurinarytractandmaleautosavedautosaved-240526080531-9d6371e3-thumbnail.jpg?width=640&height=640&fit=bounds)









































