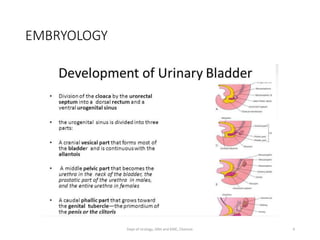
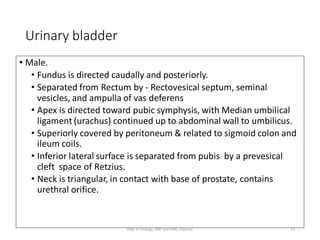
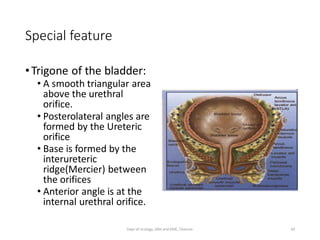
This document provides an overview of the anatomy of the urinary bladder, including its embryology, gross anatomy, histology, vascular and nerve supply, and surgical considerations. It describes the bladder's location in the pelvis, layers, relationships to surrounding organs, and changes during filling and voiding. Key structures like the trigone and bladder neck are emphasized. Modulators of bladder function from the brain and spinal cord through peripheral nerves are reviewed.


































![VENOUS DRAINAGE:
* the dorsal vein of penis passes between the
inferior pubic arch and the striated urinary
sphincter to reach the pelvis
* it trifurcates into
1. central superficial branch
2. 2 lateral plexuses (plexus of santorini)
[During retropubic prostatectomy the dorsal
vein complex is best divided distally before its
ramification to minimise blood loss.]
43
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-anatomy1-210611145958/85/Urinary-Bladder-anatomy-1-43-320.jpg)




![Neurogenic control
• Brain:
- Master control
- Conscious social control
- Frontal lobe
- Tonically inhibitory signals to detrusor.
- [Stroke,dementia,cancer, CP, parkinson, shy drager syndrome…. ]
48
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-anatomy1-210611145958/85/Urinary-Bladder-anatomy-1-48-320.jpg)

![• Sacral spinal cord:
- Primitive voiding center – Sacral reflex center – bladder contractions.
- Important intermediary between the pons and the sacral cord.
- Spinal injury: urinary frequency, urgency and urge incontinence and are
unable to empty bladder. [Detrusor sphincter dyssynergia with detrusor
hyperreflexia (DSD-DH)].
( EX … multiple sclerosis).
- Or Detrusor areflexia. (Herniated disc/ tumor)
50
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-anatomy1-210611145958/85/Urinary-Bladder-anatomy-1-50-320.jpg)
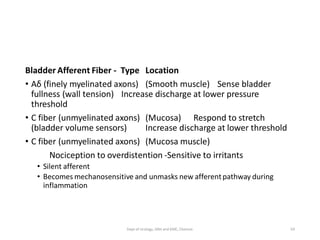
![• Peripheral nerves:
- Sympathetic: constantly active. [T10-L2].
1. Bladder to increase its capacity without increasing detrusor resting
pressure (accommodation) and stimulates the internal urinary sphincter to
remain tightly closed.
2.Sympathetic activity also inhibits para sympathetic stimulation [S2-4]
(opposite action).
51
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-anatomy1-210611145958/85/Urinary-Bladder-anatomy-1-51-320.jpg)


![• Somatic nervous system:
- External urinary sphincter and the pelvic diaphragm.
- Pudendal nerve [S2-3] originates from the nucleus of Onuf and regulates
the voluntary actions of the external urinary sphincter and the pelvic
diaphragm.
- Shy- Drager synd : Lesion in Onuf nucleus.
- Neuropraxia : after delivery- Stress incontinence.
- Suprasacral- infrapontine spinal cord trauma can cause overstimulation of
the pudendal nerve - urinary retention. SPINAL SHOCK
54
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-anatomy1-210611145958/85/Urinary-Bladder-anatomy-1-54-320.jpg)