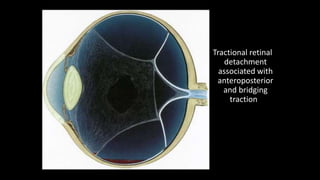
Tractional retinal detachment occurs when fibrovascular membranes exert traction on the retina, most commonly due to proliferative diabetic retinopathy or posterior segment trauma. Static traction from these membranes causes the retina to detach in a shallow, concave configuration without visible retinal breaks. Diagnosis is based on finding reduced retinal mobility and the absence of breaks, with traction visible from fibrovascular tissue. Ultrasound can help diagnose tractional detachments when the media is opaque.