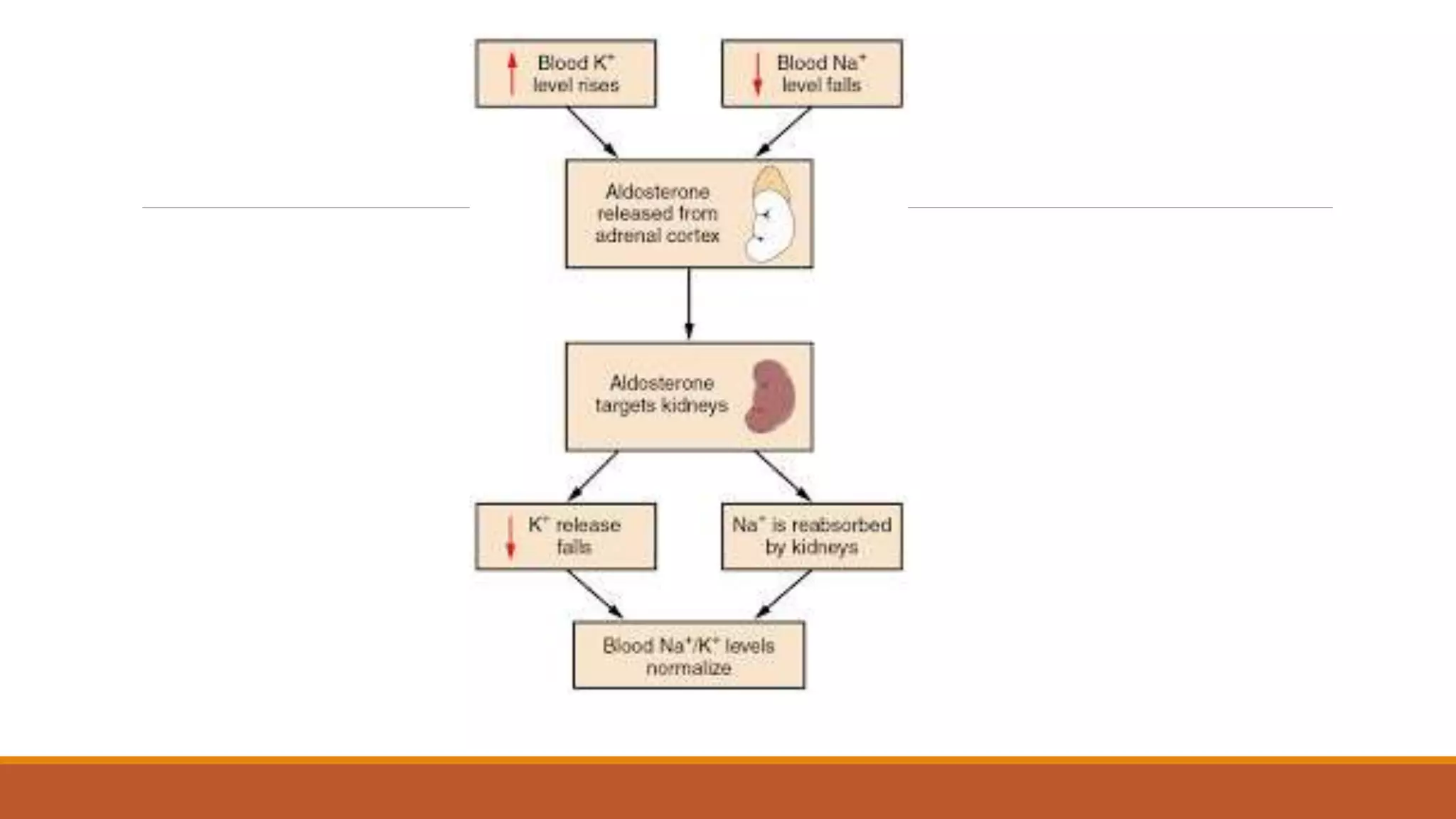
This document discusses potassium metabolism and the approach to hyperkalemia. It begins with an introduction to potassium physiology and homeostasis. The kidney plays a key role in potassium excretion, reabsorbing 85-90% in the distal tubules where regulation occurs. Hyperkalemia is defined as a serum potassium over 5.5 mEq/L and can be caused by increased potassium load, impaired excretion, or transcellular shifting. Treatment focuses on stabilizing cardiac cells, rapidly lowering potassium levels, and enhancing elimination while addressing the underlying cause. Emergency therapies include calcium gluconate, insulin therapy, beta agonists, and sodium polystyrene sulfonate.