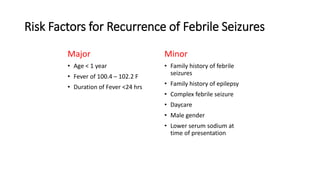
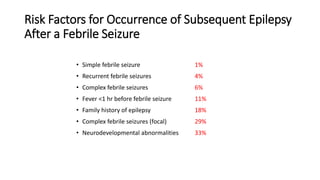
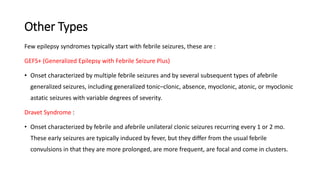
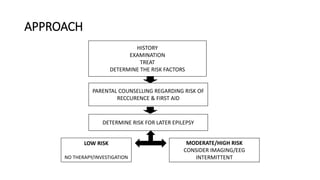
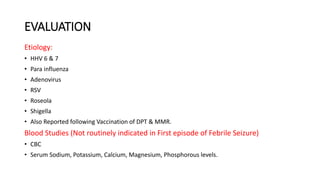
This document discusses febrile seizures in children. It defines febrile seizures as seizures accompanied by a fever between 100.4-102.2°F in children aged 6 months to 5 years without an underlying infection or metabolic imbalance. Febrile seizures are classified as simple, complex, or febrile status epilepticus based on duration and recurrence. Risk factors for recurrence and developing epilepsy later are identified. Evaluation may include bloodwork, lumbar puncture and imaging in some cases. Acute management focuses on terminating the seizure and treating the fever. Intermittent or continuous anti-seizure medication prophylaxis may be considered in children at higher risk of recurrence.














































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









