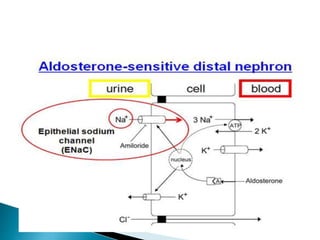
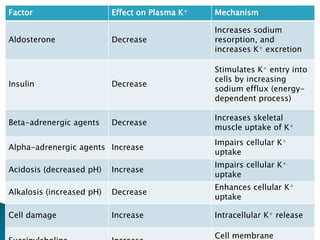
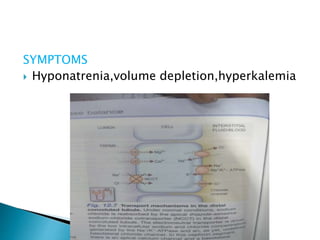
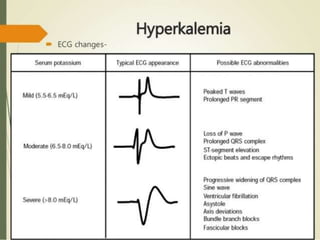
This document discusses potassium homeostasis and hyperkalemia. It notes that potassium is mainly intracellular and its serum level is tightly regulated between 3.5-5 mEq/L. Mechanisms involve sodium-potassium pumps and renal excretion. Causes of hyperkalemia include reduced renal excretion, intracellular shifts, and inadequate aldosterone levels. Symptoms range from none to muscle weakness to arrhythmias. Treatment focuses on antagonizing cardiac effects, driving potassium intracellularly, and removing excess potassium.

![ III. Inadequate excretion
A. Inhibition of the renin-angiotensin-
aldosterone axis;
(↑ risk of hyperkalemia when these drugs
are used in combination
Angiotensin-converting enzyme (ACE)
inhibitors
Renin inhibitors; aliskiren
(in combination with ACE inhibitors or
angiotensin receptor blockers [ARBs])](https://image.slidesharecdn.com/hyperkalemia-160108171542-170418195549/85/Hyperkalemia-160108171542-11-320.jpg)































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
