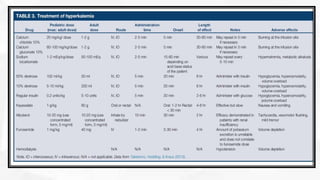
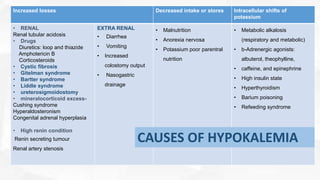
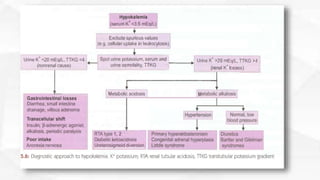
This document discusses hypokalemia and hyperkalemia. It begins by covering physiology of potassium including distribution between intracellular and extracellular spaces and homeostasis mechanisms. It then defines and describes causes and treatment of hyperkalemia including shifting potassium intracellularly or removing it. For hypokalemia it discusses increased losses, decreased intake and intracellular shifts as causes and emphasizes replacing losses. Clinical features and management focus on symptom relief and returning potassium to normal range.


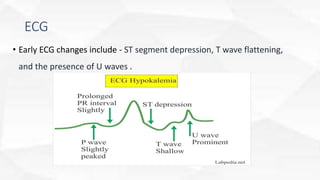






































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






