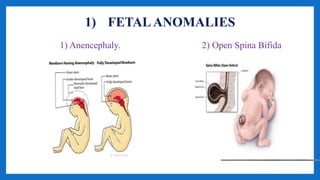
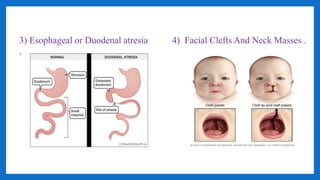
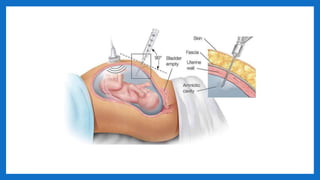
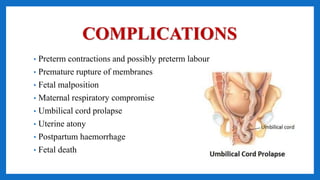
Polyhydramnios is a condition characterized by excessive amniotic fluid, exceeding 1500-2000ml, occurring in 1-2% of pregnancies and more commonly in multipara. It can result from fetal anomalies, maternal causes, placental factors, or multiple pregnancies, leading to symptoms like uterine enlargement and dyspnea. Management involves symptom relief, diagnostic tests, and could include amniocentesis or induction of labor based on the gestational period and presence of complications.




























































![metabolic disorder in pegnancy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/metabolicdisorderinpegnancyautosaved-240725113357-734a2382-thumbnail.jpg?width=640&height=640&fit=bounds)

























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


