Downloaded 469 times

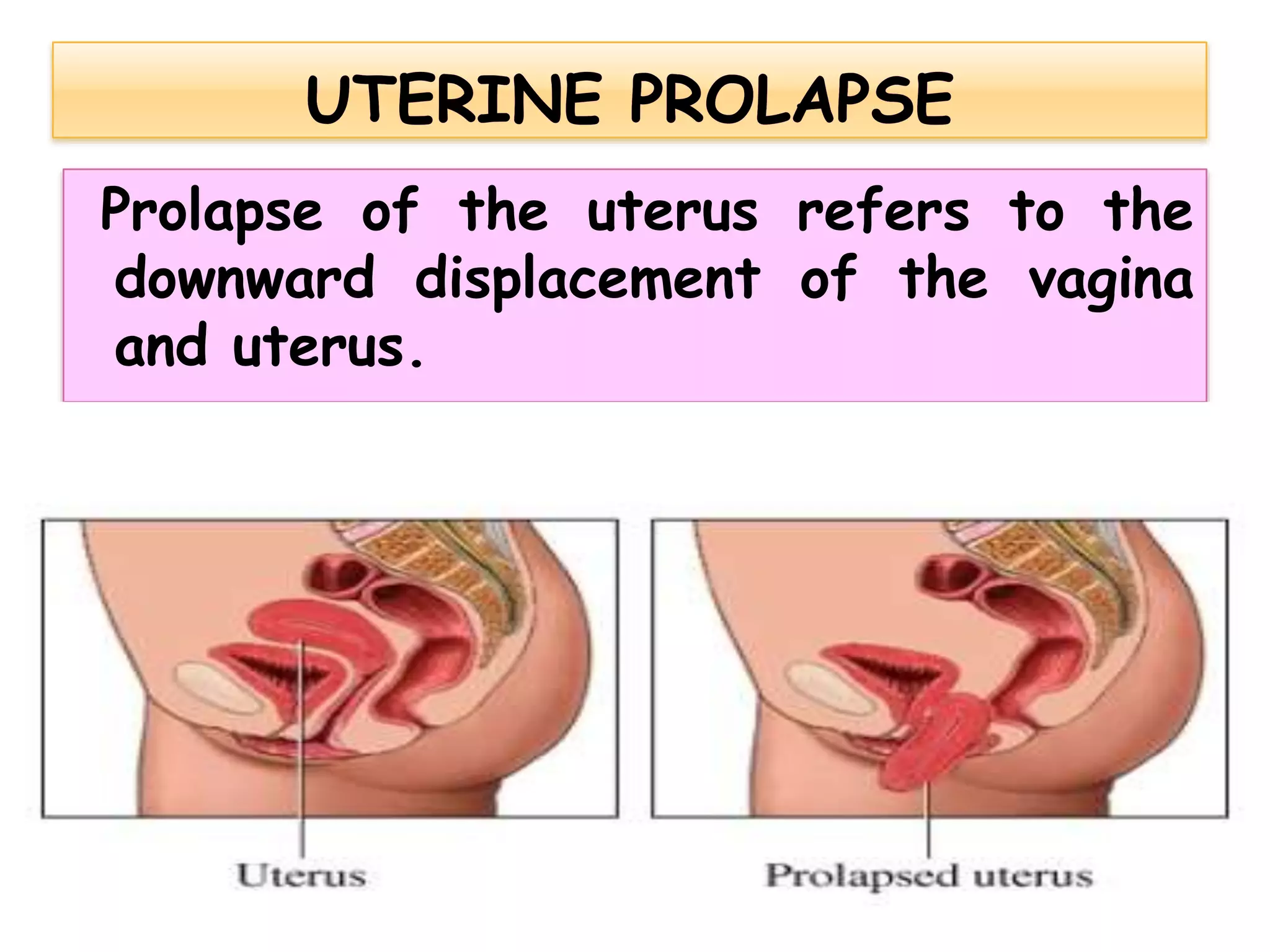
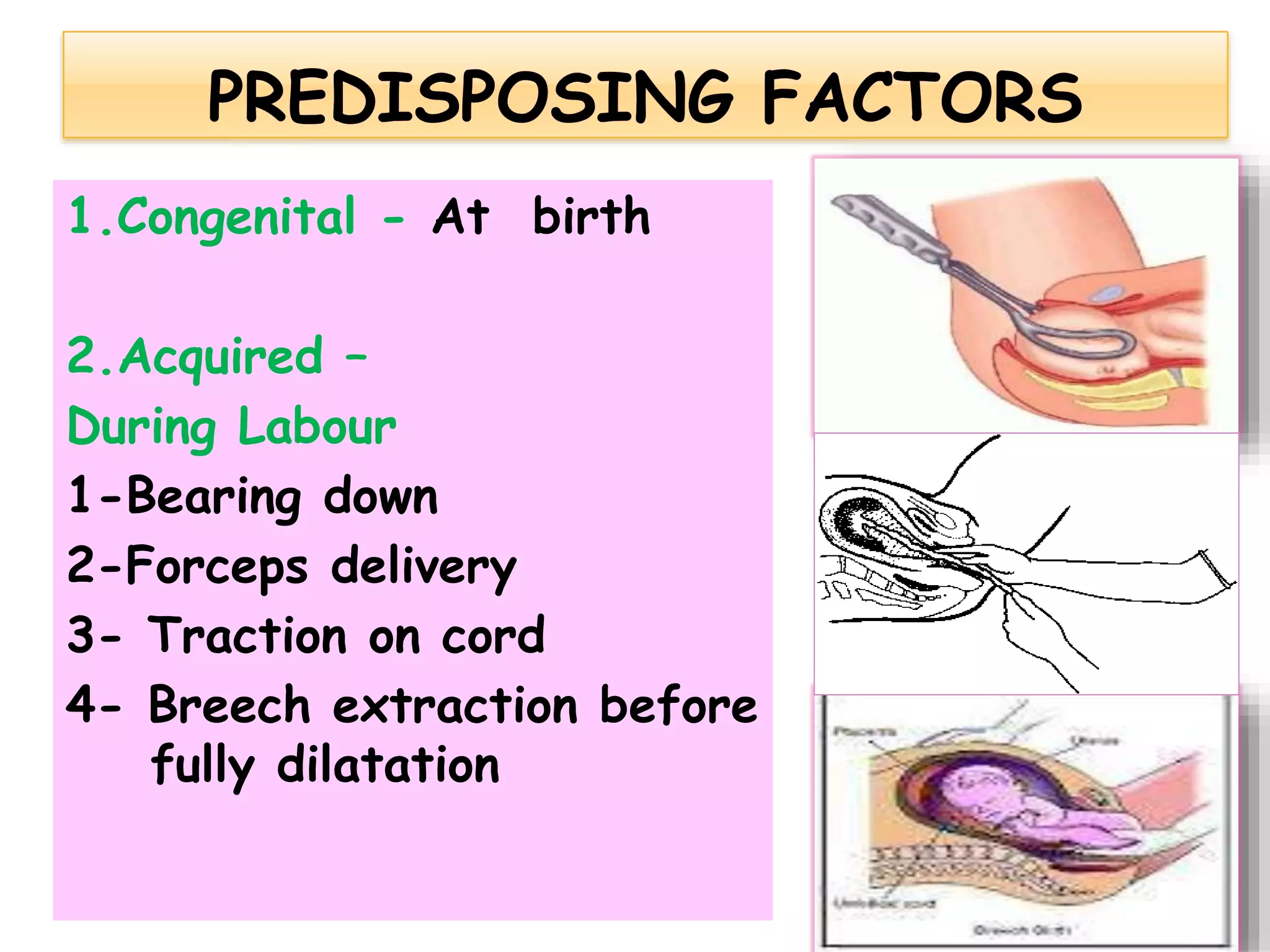







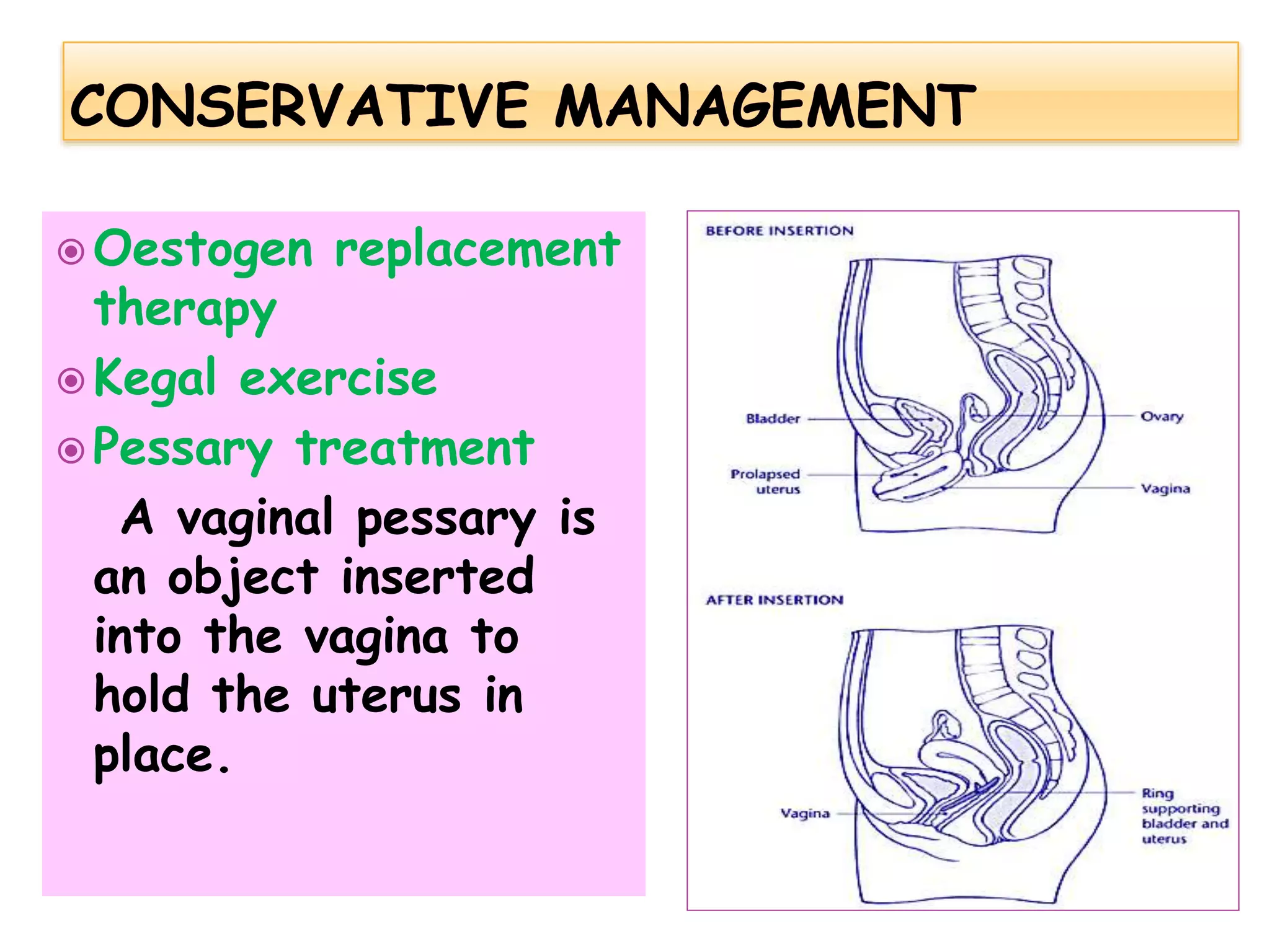





Prolapse of the uterus refers to the downward displacement of the vagina and uterus. It can be congenital or acquired due to factors like childbirth, obesity, chronic coughing, and uterine fibroids. Symptoms include feeling something coming down in the vagina, backache, difficulty urinating, and incomplete bowel movements. Diagnosis involves physical examination in both dorsal and standing positions. Management includes preventative measures, conservative options like pessaries and exercises, and surgery if symptoms become worse.








































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










