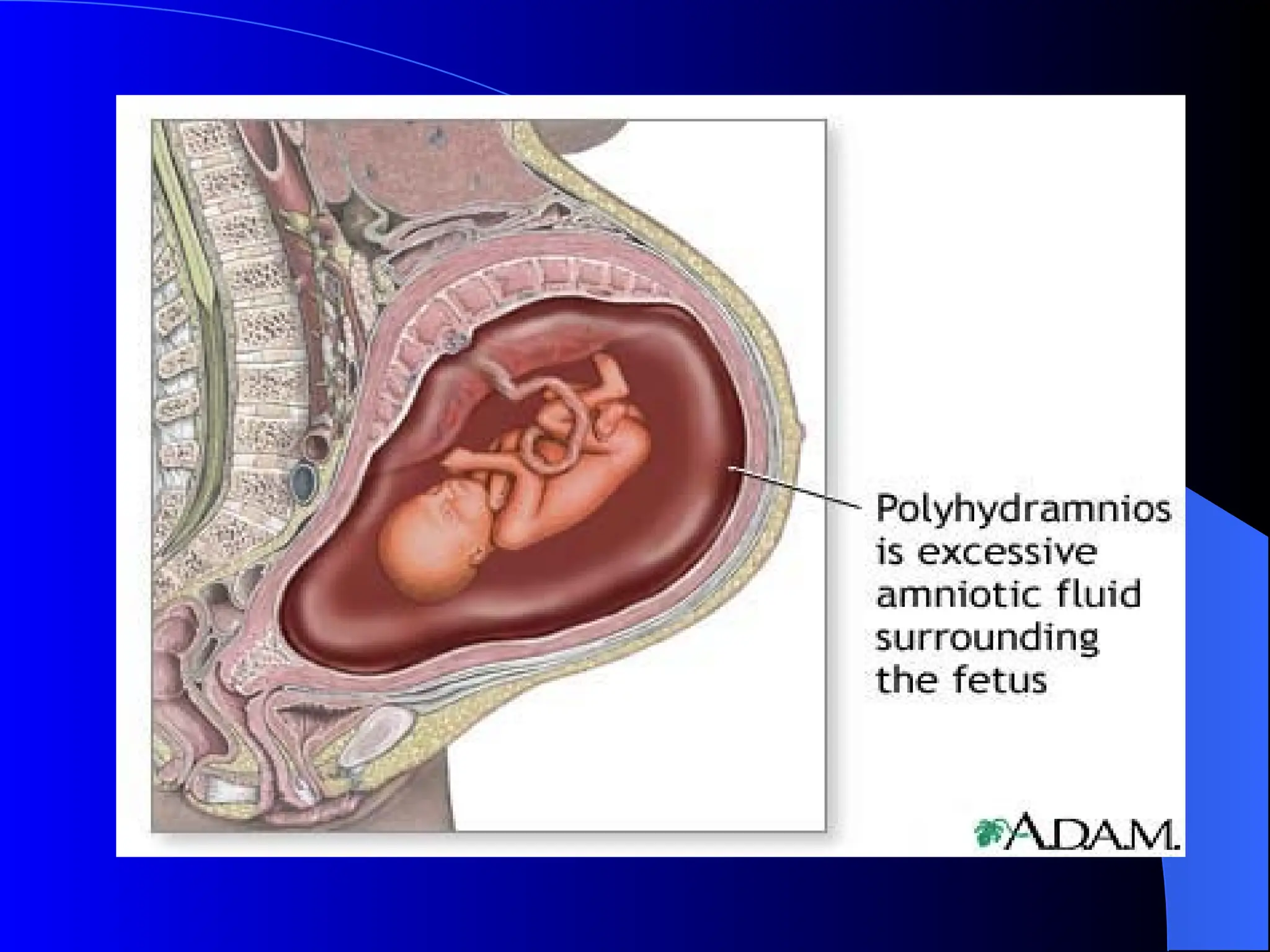
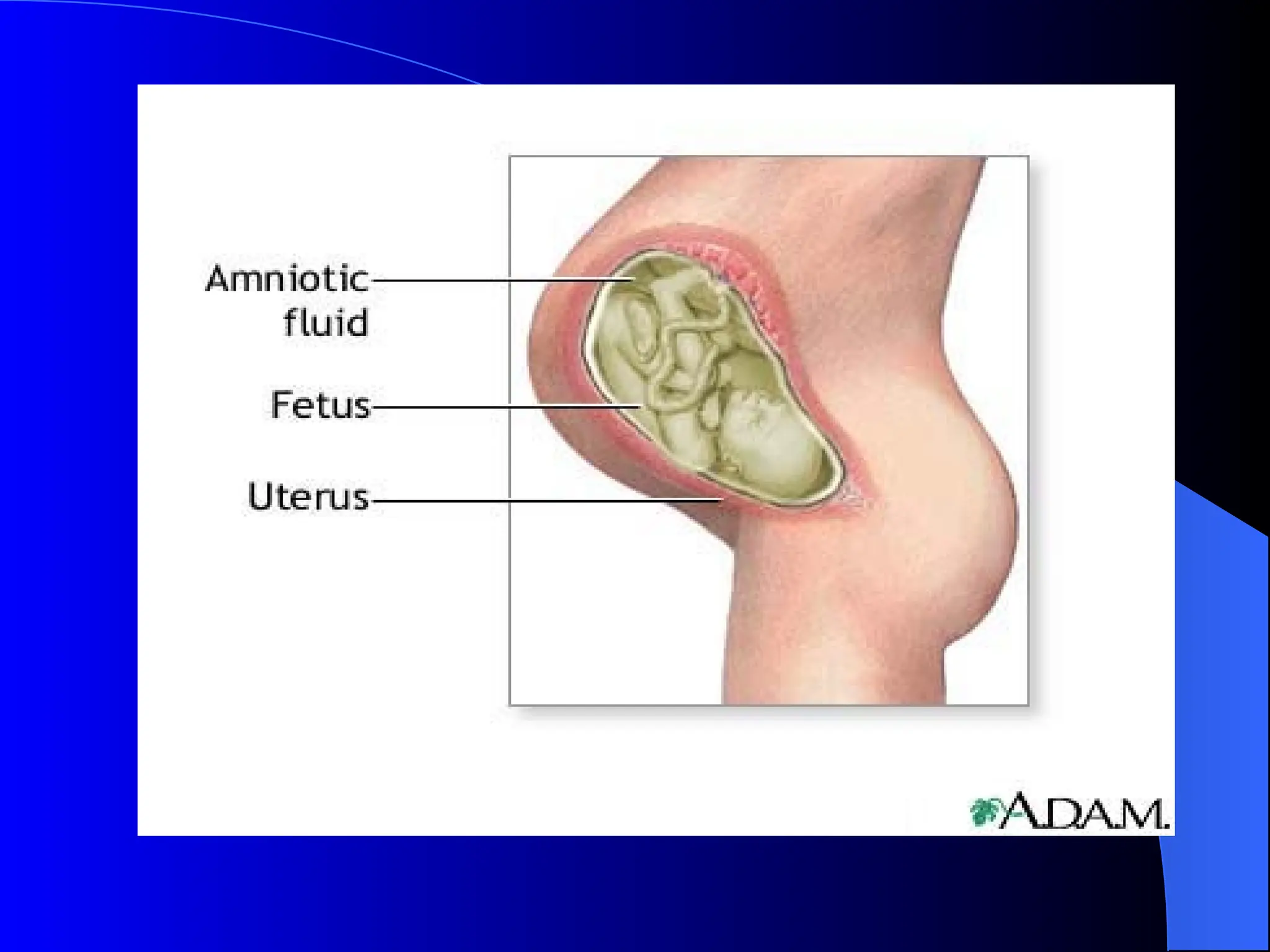
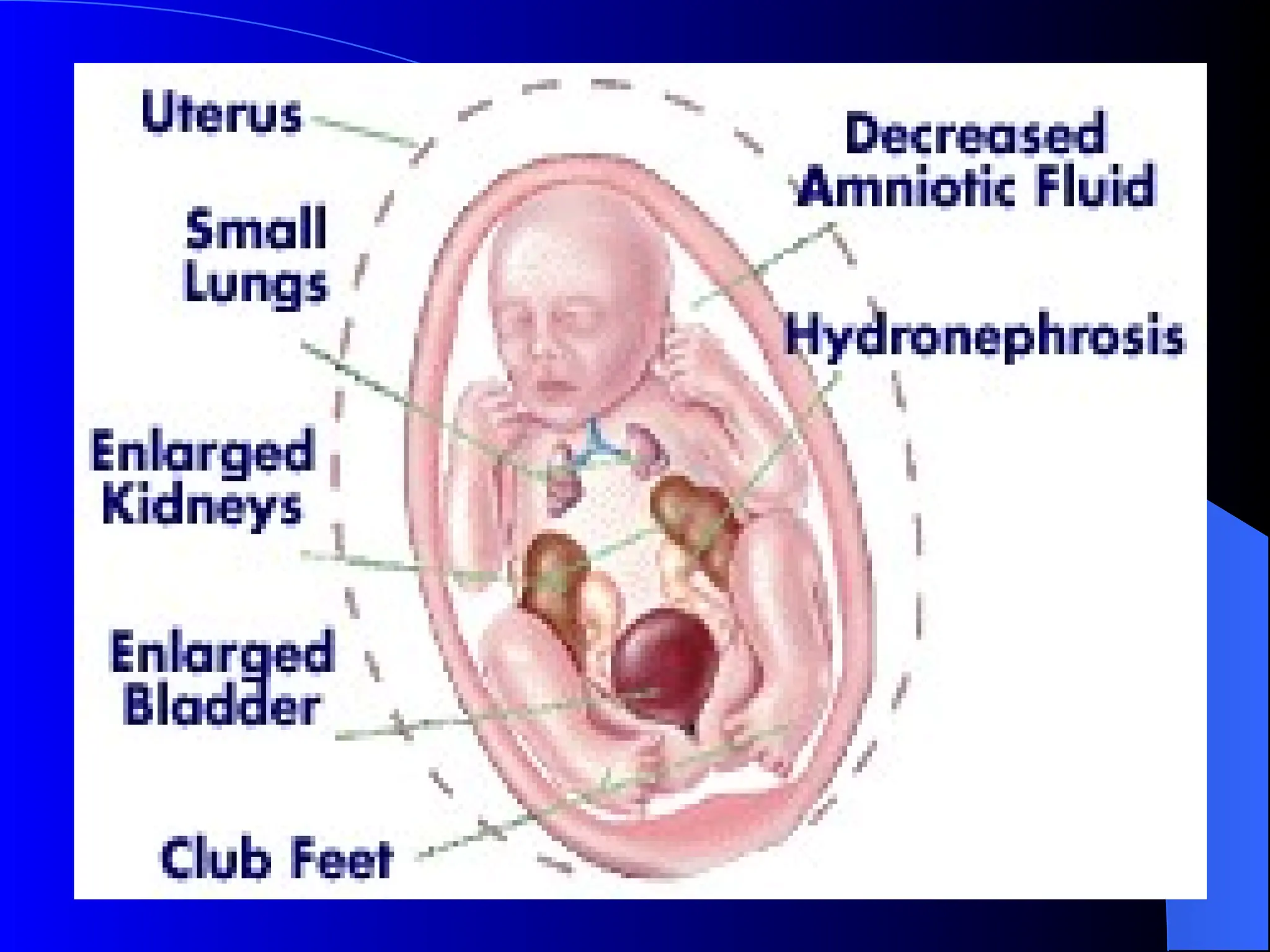
The document discusses the physiology, definitions, etiologies, symptoms, diagnosis, and treatment of polyhydramnios and oligohydramnios. Polyhydramnios is characterized by excess amniotic fluid, with potential causes including fetal anomalies and diabetes, while oligohydramnios involves insufficient amniotic fluid, often leading to severe fetal complications. Treatment approaches vary, with mild cases of polyhydramnios requiring little intervention and oligohydramnios often necessitating delivery or amnioinfusion.