Polyhydramnios and Oligohydramnios topic presented in detail. Causes maternal and fetal risks, antenatal care, intrapartum and postpartum care, maternal and fetal complications and management, pathophysiology
Wisdom
Truth
Motto Vision; The
Dream/Tomorrow
To impart evidence based
research oriented medical
education
To provide best possible
patient care
To inculcate the values of
mutual respect and ethical
practice of medicine
Learning Objectives
toenable students understand importance
of amniotic fluid for fetal well being
Causes of liquor abnormalities
Complications associated with
oligohydramnios and polyhydramnios
Management of liquor abnormalities
6.
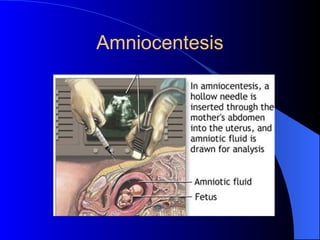
Amniotic fluid
Early pregnancy:Amnion
10th
week: Transudate of the fetal serum
via skin & umbilical cord
From 16th
week: Fetal skin becomes
impermeable to water
Contribution of fluid through
the kidneys & lungs and
removal by fetal swallowing
Amniotic fluid volume
Progressiveincrease from 10-38th
week
10 weeks: 30 ml
20 weeks: 300 ml
30 weeks: 600 ml
38 weeks: 1000ml
From 38th
week onwards: rapid fall
40 weeks: 800 ml
42 weeks: 350 ml
9.
Measurement
Two ways
1. Themaximum vertical pool (MVP)
2. Amniotic fluid index (AFI)
MVP : After a general survey
Less than 2 cm
Greater than 8cm
10.
Amniotic fluid index
Uterusis divided in four quadrants
A vertical measurement is taken of the
deepest pool of fluid that is free of
umbilical cord in all the four quadrants of
the uterus and is summated
Third trimester: 10-25 cm
Below 5 cm. (less)
Above 25 cm (more)
11.
The function ofthe amniotic
fluid
Protect the fetus from mechanical injury
Permit movement of the fetus while
preventing limb contracture
Prevent adhesions between fetus & amnion
Permit fetal lung development in which
there is two-way movement of fluid into
fetal bronchioles
Absence of AF: pulmonary hypoplasia
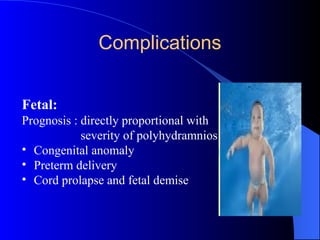
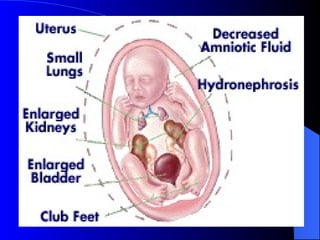
Complications
• Extremely poorfetal prognosis, especially
in early pregnancy
• Adhesions between amnion and fetal parts
---malformations and amputations
• Musculoskeletal deformities
• Pulmonary hypoplasia
29.
Cord Compression-- >fetal hypoxia
Passage of meconium into low AF volume:
thick particulate suspension -->respiratory
compromise
Fetal demise
Iatrogenic preterm delivery/cesarean
Vertical
integration
Beneficence
• TAKE
HOME
MESSAGE
The principleof beneficence is the obligation of physician to act for
the benefit of the patient and supports a number of moral rules to
protect and defend the right of others, prevent harm, remove
conditions that will cause harm, help persons with disabilities, and
rescue persons in danger.
It is worth emphasizing that, the language here is one of positive
requirements. The principle calls for not just avoiding harm, but
also to benefit patients and to promote their welfare.
35.
Ethical Consideration
Councelling (anomaly,fetal prematurity,
still birth ,pregnancy outcome)
Termination of pregnancy ( fetamaternal
indication)
Mode and time of delivery
Implications on future pregnancy
36.
References
1. Obsterics byten teachers. Louise C. Kenny, Jenny E. Myers. 20th
ed
ISBN 9781498744393. Published June 1, 2017 by CRC Press
2. Polyhydramnios: Causes, Diagnosis and Therapy
A. Hamza,1
D. Herr,1
E. F. Solomayer,2
and G. Meyberg-Solomayer1
Geburtshilfe Frauenheilkd. 2013 Dec; 73(12): 1241–1246.
doi: 10.1055/s-0033-1360163
3. Amnioreduction procedure for singleton pregnancies complicated by
polyhydramnios causing maternal discomfort
B.S. Albaqawi, A.S. Alghamdi, M.M. Abuzaid, W.Y. Alaali, B.I. Sallout
First published: 08 September 2016
https://doi.org/10.1002/uog.17097
38.
mcqs
1. a24year old primigravida obeses BMI 35Kg/m2presents for first
antenatal booking .she is 26 weeks, her SFH is 36cm and tense
abdomen.what is ur next best step in management?
a. admit for blood sugar monitoring
b. Inquire about LMP
c. ultrasound anomaly +liq,and blood sugar monitoring
d. expectant management
e. induce labor
39.
1. a24year old primigravida obeses BMI 35Kg/m2presents for first
antenatal booking .she is 26 weeks, her SFH is 36cm and tense
abdomen.what is ur next best step in management?
a. admit for blood sugar monitoring
b. Inquire about LMP
c. ultrasound for anomaly+liq and blood sugar monitoring
d. expectant management
e. induce labor
40.
2. aG2P1 at 37 weeks presents for checkup.She is known
hypertensive since 4 years.Her SFH IS 32cm,long cephalic with good
fetal heart beats,EFW is 3.1kg.Ultrasound shows almost nil
liquor.bishop score is 9.How will you manage her?
a. b.p monitoring,dopplersultrasound.
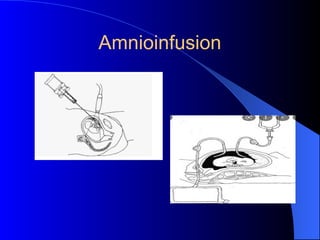
b. Amnioinfusion
c. steriod cover and induce labor
d. emergency cesarean section
e. Expectant managment
41.
2. aG2P1 at 37 weeks presents for checkup.She is known
hypertensive since 4 years.Her SFH IS 32cm,long cephalic with good
fetal heart beats,EFW is 3.1kg.Ultrasound shows almost nil
liquor.bishop score is 9.How will you manage her?
a. b.p monitoring,dopplersultrasound.
b. Amnioinfusion
c. steriod cover and induce labor
d. emergency cesarean section
e. Expectant managment










































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













