AMNIOTIC FLUID
This isfluid that surrounds the fetus in the womb
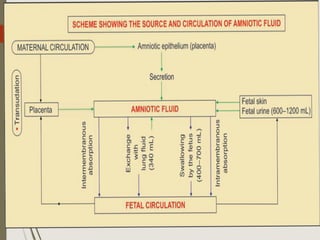
SOURCE:
(1) Fetal:
a. Active secretion from the amniotic epithelium.
b. Transudation from the fetal circulation.
c. Fetal urine.
(2) Maternal :
Transudation from maternal circulation.
The fetal origin contributes more in the production of the amniotic
fluid.
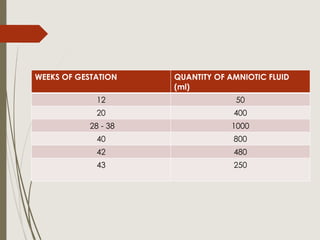
It isabout 400 ml at mid pregnancy, reaches about 1000
ml at 36-38 weeks
-Then decreases later on to be scanty in post-term
pregnancy.
It has a low It is a clear pale, slightly alkaline ( pH 7.2)
fluid.
SG of 1.010
It becomes highly hypotonic to maternal serum at term
pregnancy.
- An osmolarity of 250mOsmol/l is suggestive of fetal
maturity; and osmolality falls with advancing age.
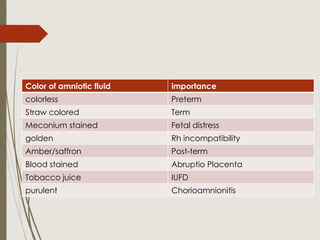
Color of amnioticfluid importance
colorless Preterm
Straw colored Term
Meconium stained Fetal distress
golden Rh incompatibility
Amber/saffron Post-term
Blood stained Abruptio Placenta
Tobacco juice IUFD
purulent Chorioamnionitis
8.
COMPOSITION
Water (98-99%),
carbohydrates ( glucose and fructose),
proteins ( albumin and globulins),
lipids,
hormones (oestrogen and progesterone),
enzymes (alkaline phosphatase),
minerals (sodium, potassium and chloride),
suspended materials as vernix caseosa, lanugo hair,
desquamated
epithelial cells and meconium.
9.
Circulation of amnioticFluid:
The amniotic fluid is not in a static state but is in a
continuous turn over, 500 ml of it are replaced each hour.
10.
Functions:
During pregnancy:
1. Protectsthe fetus against injury.
2. A medium for free foetal movement.
3. Maintains the foetal temperature.
4. Source for nutrition of the fetus.
5. A medium for foetal excretion.
11.
During Labour:
1. Thefore-bag of water helps the dilatation of the cervix
during labour.
2. It acts as an antiseptic for the birth canal after rupture of
the membranes.
POLYHYDRAMNIOS/HYDRAMNIOS:
Anatomically, it’sa state where liquor amni is >2,000ml.
Clinically, Its excessive accumulation of liquor amnii
causing discomfort to the patient &/or when an imaging
help is needed to make a diagnosis of the lie & fetus
presentation.
This occurs in fewer than 1 % of the pregnancies
Sonographic diagnosis is made when amniotic fluid
index is >24cm (95th
centile of gestational age) & a
deepest vertical pocket is >8cm.
14.
About halfof all cases of Polyhydramnios are idiopathic
the rest are due to maternal diabetes or congenital
malformation.
Early diagnosis of Polyhydramnios is performed during
pregnancy, a diabetic screen and a thorough fetal
ultrasound should be performed. In particular, the fetal size
should be determined, the amniotic fluid quantified, the
gastrointestinal tract should be imaged, and a biophysical
profile should be performed to verify normal tone,
movement and breathing.
15.
Polyhydramnios ismore likely to occur when:
There is a multiple gestation.
There is maternal diabetes.
There is a congenital malformation
16.
ETIOLOGY OF POLYHYDRAMNIOS
Itmay be the result of deficient absorption as
well as excessive production of liquor amnii,
which may be temporary or permanent.
The composition of the liquor amnii,
however, remains normal.
17.
Congenital fetal malformations(structural and
chromosomal) are associated with polyhydramnios in
about 20% cases.
i. Anencephaly
18.
ii.Open spina bifida
iii.Esophageal or duodenal atresia
iv.Facial clefts and neck masses
V. Aneuploidy and genetic syndrome.
CLINICAL TYPES: Dependingon the rapidity of onset,
hydramnios may be:
(a) Chronic (most common), onset is insidious taking few
weeks.
(b) Acute (extremely rare)—onset is sudden, within few
days or may appear acutely on pre-existing chronic
variety. The chronic variety is 10 times more common than
the acute one.
Polyhydramnios may be—(a) mild: DVP more than 8–11
cm (b) moderate: DVP: 12–15 cm and
(c) severe: DVP more than or equal to 16 cm.
22.
CHRONIC POLYHYDRAMNIOS
In themajority of cases, the accumulation of liquor is gradual
and as such, the patient is not very much
inconvenienced.
SYMPTOMS: The symptoms are mainly from mechanical
causes.
-Respiratory—The patient may suffer from dyspnea or even
remain in the sitting position for
easier breathing.
-Palpitation
- Edema of the legs, varicosities in the legs or vulva and
hemorrhoids.
SIGNS:
-The patient may be in a dyspneic state in the lying down
position.
-Evidence of preeclampsia (edema, hypertension and
proteinuria) may be present
23.
I. ABDOMINAL EXAMINATION
Inspection:
Abdomenis markedly enlarged, looks
globular with fullness at the flanks.
The skin is tense, shiny with large striae. Everted umbilicus.
Palpation:
Height of the uterus is more than the
period of amenorrhea.
Girth of the abdomen round
Fetal parts cannot be well-defined; so also
the presentation or the position. External
ballottement can be elicited more easily.
Auscultation: Fetal heart sound is not heard
distinctly, although its presence can be picked up by Doppler
Ultrasound.
24.
INTERNAL EXAMINATION:
The cervixis pulled up, may be partially taken up or at
times, dilated, to admit a fingertip through which tense
bulged membranes can be felt.
25.
INVESTIGATIONS:
a).Sonography: Sonography ishelpful;
(1) to detect abnormally large echo-free space
between the fetus and the uterine wall.
(2) to exclude multiple fetuses,
(3) to note the presentation of the fetus,
(4) to diagnose any fetal congenital malformation.
26.
b.Blood:
(1) ABO andRh grouping — Rhesus isoimmunization
may cause hydrops fetalis and fetal ascites.
(2) Postprandial sugar and if necessary glucose
tolerance test.
C. Amniotic fluid: Estimation of alpha fetoprotein which
is markedly elevated in the presence of a
fetus with an open neural tube defect.
1. Twins:The diagnosis is often confused and
difficult because of its association with
hydramnios because Abdomen is markedly
enlarged, too many fetal parts, fluid thrill absent.
2. Pregnancy with huge ovarian cyst: The gravid
uterus can be felt separate from the cyst, internal
examination shows the cervix to be pushed down
into the pelvis. In hydramnios, the lower segment
has to ride
above the pelvic brim, so that the cervix is drawn
up, X-ray of the abdomen or sonography is
helpful.
29.
3. Maternal ascites:
(i)Presence of shifting dullness,
(ii) resonance on the midline due to floating gut whereas
in hydramnios, it becomes dull
(iii) internal examination and palpation of the normal
size uterus, if possible, can give the clue
(iv) straight X-ray of the abdomen or sonography helps
to exclude pregnancy.
30.
MANAGEMENT
Recently there hasbeen a falling trend in the incidence
of hydramnios of severe magnitude. The reasons are:
(1) Early detection and control of diabetes.
(2) Rhesus isoimmunization is now preventable].
(3) Genetic counseling in early months and detection of
fetal congenital abnormalities with ultrasound and their
termination, reduce their number in late pregnancy.
31.
COMPLICATIONS
The complications ofhydramnios are grouped into:
Maternal and Fetal
Maternal:
During pregnancy—There is increased incidence of:
(1) Preeclampsia (25%)
(2) Malpresentation and persistence of floating head
(3) Premature rupture of the membranes
(4) Preterm labor
(5) Accidental hemorrhage due to decrease in the
surface area of the emptying uterus beneath the
placenta, following sudden escape of liquor amnii.
32.
During labor:
(1) Earlyrupture of the membranes
(2) Cord prolapse
(3) Uterine inertia
(4) Increased operative delivery due to malpresentation
(5) Retained placenta, postpartum
hemorrhage and shock. The postpartum hemorrhage is
due to uterine atony.
Puerperium:
(1) Subinvolution
(2) Increased puerperal morbidity due to infection
resulting from increased operative interference and
blood loss.
33.
Fetal: There isincreased perinatal mortality to the extent
of about 50%. The deaths are mostly due to prematurity
and congenital abnormality (40%).
Other contributing factors are cord prolapse, hydrops
fetalis, effects of increased operative delivery and
accidental hemorrhage.
34.
Treatment of polyhydramniosis usually tailored
according to the underlying cause.
MILD POLYHYDRAMNIOS (DVP: 8–11 cm): It is
commonly found in midtrimester and usually requires
no treatment, except extra bed rest for a few days. The
excess liquor is expected to be diminished as
pregnancy advances (transient).
SEVERE POLYHYDRAMNIOS (DVP: ≥16 cm): In view
of the risks involved and the high perinatal
mortality rate, the patient should be shifted in a hospital
equipped to deal with “high-risk” patients.
Principles:
(1) To relieve the symptoms
(2) To find out the cause
(3) To avoid and to deal with the complication
35.
Polyhydramnios may be
(a)transient where LVP returned to normal with
progress of pregnancy or
(b) persistent cases with persistent polyhydramnios need
investigations for congenital fetal anomalies,
genetic syndromes and also need close monitoring.
Supportive therapy includes bed rest, if necessary, with
a back rest and treatment of the associated
conditions like preeclampsia or diabetes on the usual
line.
The use of diuretic is of little value.
Sulindac (COX-2 inhibitor), 200 mg every 12 hours,
(under supervision) has been found to be most effective
in unexplained cases. It has been found to decrease
amniotic fluid as it reduces fetal urine output.
36.
Further management dependson:
(1) Response to treatment
(2) Period of gestation
(3) Presence of fetal malformation
(4) Associated complicating factors.
A.Uncomplicated cases: (No demonstrable fetal
malformation)
1. Response to treatment is good: The pregnancy is to be
continued awaiting spontaneous delivery at term.
2. Unresponsive: (with maternal distress).
(a) Pregnancy less than 37 weeks: An attempt is made to
relieve the distress with a hope of continuation of pregnancy by
amniocentesis (amnio reduction).
37.
Slow decompression isdone at the rate of about 500 mL per hour and
the amount of fluid to be removed should be sufficient enough to
relieve the mechanical distress. Normally amnio drainage is stopped
when the AFI is less than 25 cm. Because of slow decompression,
chance of accidental hemorrhage is less but liquor amnii may again
accumulate, for which the procedure may have to be repeated.
Amniotic fluid can be tested for fetal lung maturity
.
(b)Pregnancy more than 37 weeks: Induction of labor is done .
The following procedures may be helpful.
Amniocentesis --drainage of good amount of liquor ----to check the
favorable lie and presentation of the fetus --a stabilizing oxytocin
infusion is started---low rupture of the membranes is done when the
lie becomes stable and the presenting part gets fixed to the pelvis.
This will minimize sudden decompression with separation of the
placenta, change in the lie of the fetus and cord prolapse.
38.
B.With congenital fetalabnormality:
Referral to a maternal fetal medicine unit should ideally be
done. When decision for termination is made, it is to be done
irrespective of duration of pregnancy.
Amniocentesis is done to drain good amount of liquor.
Thereafter induction by vaginal PGE2 gel insertion followed by
low rupture of membranes is done.
If, accidentally, low rupture of the membranes occurs, escape
of gush of liquor should be immediately controlled by placing
the palm over the introitus to
avoid accidental hemorrhage. The lie should be checked and if
found longitudinal, oxytocin infusion
may be started
39.
DURING LABOR:
. Internalexamination should be done soon after the
rupture of the membranes to exclude cord prolapse.
If the uterine contraction becomes sluggish, oxytocin
infusion may be started, if not contraindicated.
To prevent postpartum hemorrhage, intravenous
methergine 0.2 mg should be given with the delivery
of the anterior shoulder. One must remain vigilant
following the birth of the baby for retained placenta,
postpartum hemorrhage and shock. Baby should be
thoroughly examined for any congenital anomaly.
40.
ACUTE POLYHYDRAMNIOS
Acute hydramniosis extremely rare. The onset is acute and the
fluid accumulates within a few days. It usually occurs before 20
weeks of pregnancy. It is usually associated with monozygotic
twins with TTTS or chorioangioma of the placenta.
SYMPTOMS: Features of acute abdomen predominate—such as
abdominal pain, nausea and vomiting.
SIGNS: The patient looks ill, Absence of features of shock,
Edema of the legs or presence of other associated features of
preeclampsia, Abdomen is hugely enlarged more than the period
of amenorrhea; the wall is tense with shiny skin, Fluid thrill is
present, Fetal parts cannot be felt nor is the fetal heart sound
audible, Internal examination reveals—taking up of the cervix or
even dilatation of the os through which the bulged membranes
are felt, Sonography shows multiple fetuses or at times fetal
abnormalities
41.
TREATMENT:
Most often, spontaneousabortion occurs. In case
with severe TTTS, repetitive amnioreduction until the
AFI is normal, may improve the perinatal outcome.
Laser ablation may cure the cause of TTTS whereas
amnioreduction only treats the symptoms
42.
OLIGOHYDRMNIOS
Oligohydrmnios thisis defined as having less than
200 ml of amniotic fluid at term or an AFI of less than
5 cm. oligohydrmnios occurs in 8.2% of antepartum
patients, in 38% of labouring patients and is
associated with significantly increased perinatal
morbility and mortality. Diabetes is commonly thought
of as a reason for Oligohydrmnios
43.
ETIOLOGY
A. Fetal conditions:
(i)Fetal chromosomal or structural anomalies
(ii) Renal agenesis
(iii) Obstructed uropathy
(iv) Spontaneous rupture of the membrane
(v) Intrauterine infection
(vi) Drugs: PG inhibitors, ACE inhibitors
(vii) Postmaturity
(viii) IUGR
(ix) Amnion nodosum (failure of secretion by the cells of the amnion
covering the placenta).
B. Maternal conditions:
(i) Hypertensive disorders
(ii) Uteroplacental insufficiency
(iii) Dehydration
(iv) Idiopathic.
44.
DIAGNOSIS:
(1) Uterine sizeis much smaller than the period of
amenorrhea
(2) Less fetal movements
(3) The uterus is “full of fetus” because of scanty liquor (4)
Malpresentation (breech) is common
(5) Evidences of intrauterine growth retardation of the fetus
(6) Sonographic diagnosis is made when
largest liquor pool is less than 2 cm. Ultrasound visualization
is done following amnioinfusion of 300
mL of warm saline solution
(7) Visualization of normal filling and emptying of fetal
bladder essentially rules out urinary tract abnormality.
(8) Oligohydramnios with fetal symmetric growth restriction is
associated with increased chromosomal abnormality.
45.
COMPLICATIONS
Fetal:
(1) Abortion
(2) Deformitydue to intra-amniotic adhesions or due to
compression.
(3)still birth
(4) Cord compression
(5) High fetal mortality.
Maternal:
(1) Prolonged labor
(2) Increased operative interference due to
malpresentation.
46.
TREATMENT: Presence offetal congenital
malformation needs referral to a fetal medicine unit.
When decision for delivery is made, it should be
done irrespective of the period of gestation. Isolated
oligohydramnios in the third trimester with a normal
fetus may be managed conservatively.
Oral administration of water increases amniotic fluid
volume. In labor, cord compression is common.
Amnioinfusion (prophylactic or therapeutic) for
meconium liquor is found to improve neonatal
outcome.
47.
In theearly pregnancy there is the worry of
amniotic adhesions causing deformities or
constriction of the umbilical cord. There is also
concern about pressure deformities, like clubfeet
due to not having enough free space in the
womb.
Can also lead to compression of the cord, which
can result to fetal hypoxial, meaning that the
baby is not getting enough oxygen.
48.
There aremany factors that need to be taken into
consideration.
Meconium, if passed cannot be diluted in cases of
true oligohydramnios, however there is an increase in
the numbers of babies having foetal distress requiring
a caesarean birth



![MANAGEMENT
Recently there has been a falling trend in the incidence
of hydramnios of severe magnitude. The reasons are:
(1) Early detection and control of diabetes.
(2) Rhesus isoimmunization is now preventable].
(3) Genetic counseling in early months and detection of
fetal congenital abnormalities with ultrasound and their
termination, reduce their number in late pregnancy.](https://image.slidesharecdn.com/abnormalitiesofamnioticfluid-250819184656-d7142226/85/ABNORMALITIES-OF-AMNIOTIC-FLUID-obs-pptx-30-320.jpg)