Downloaded 2,035 times
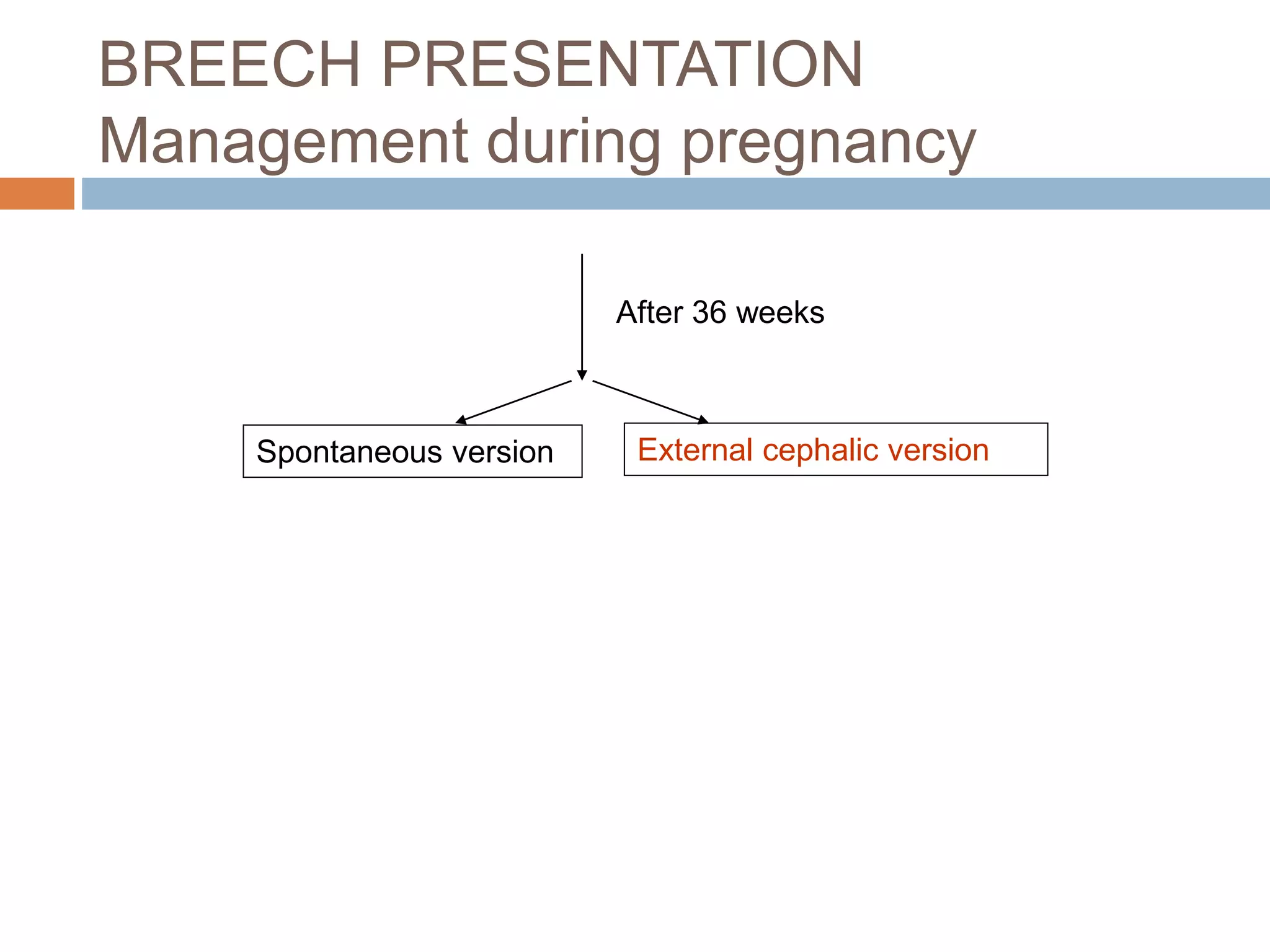
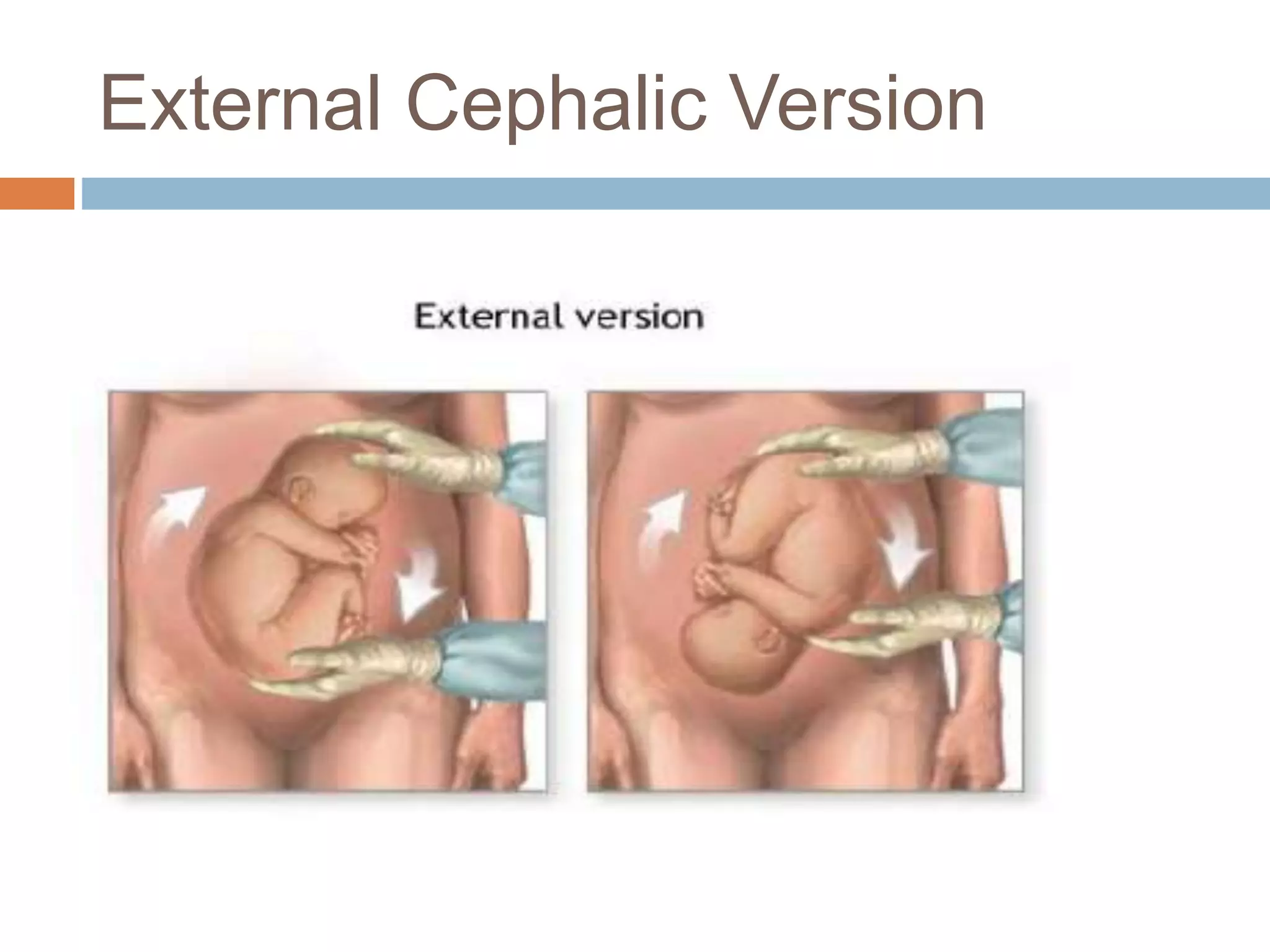
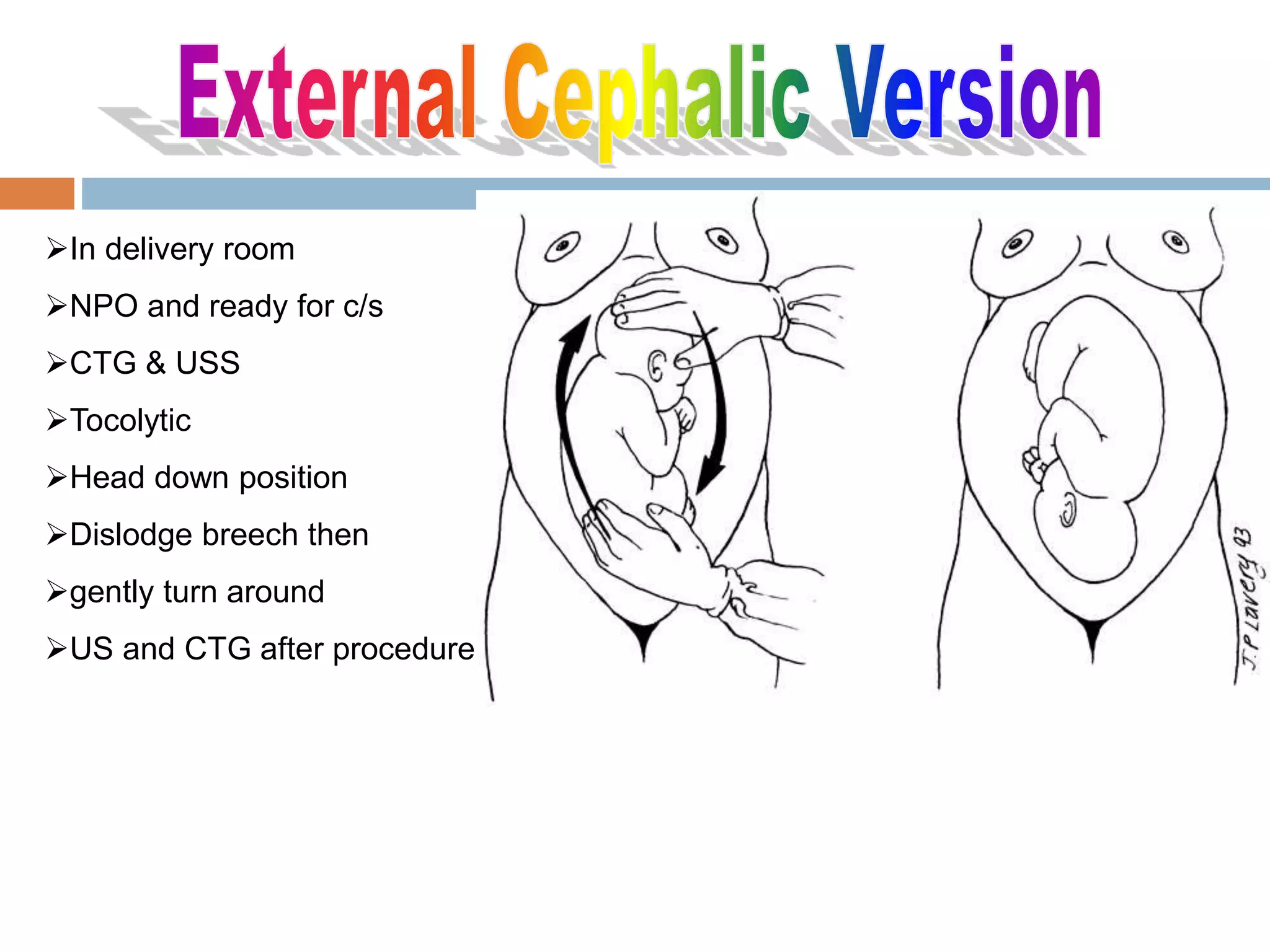
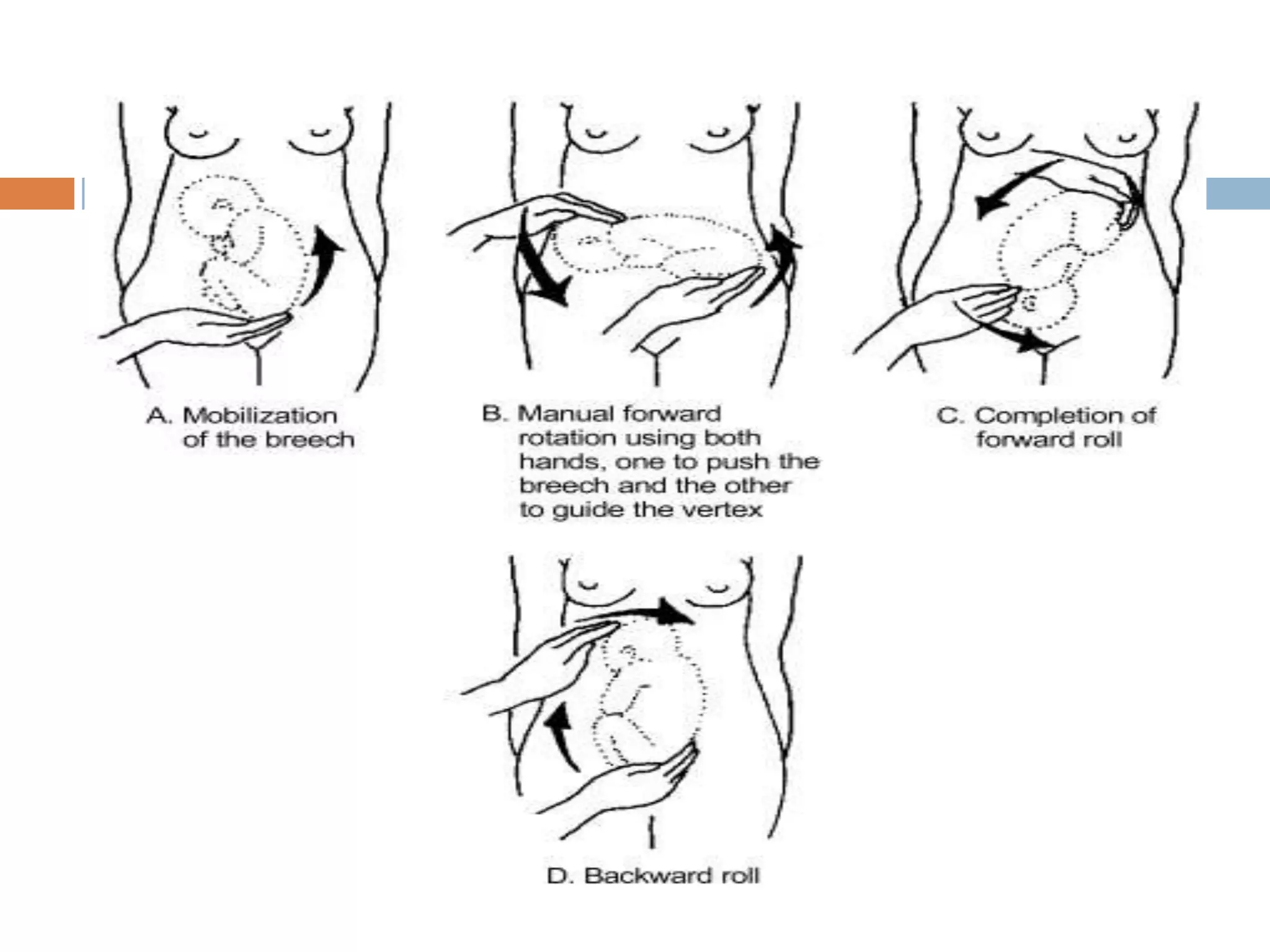
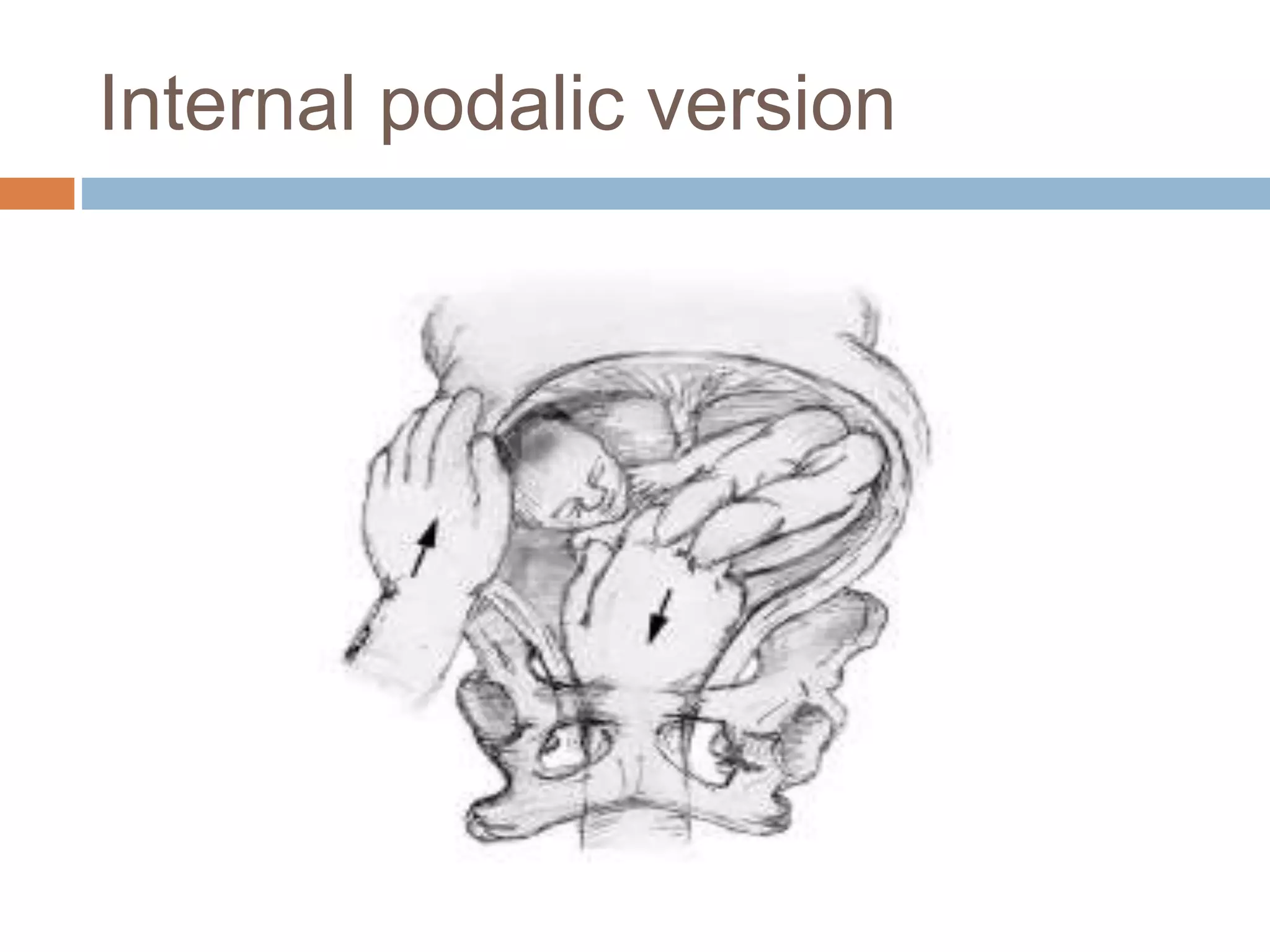
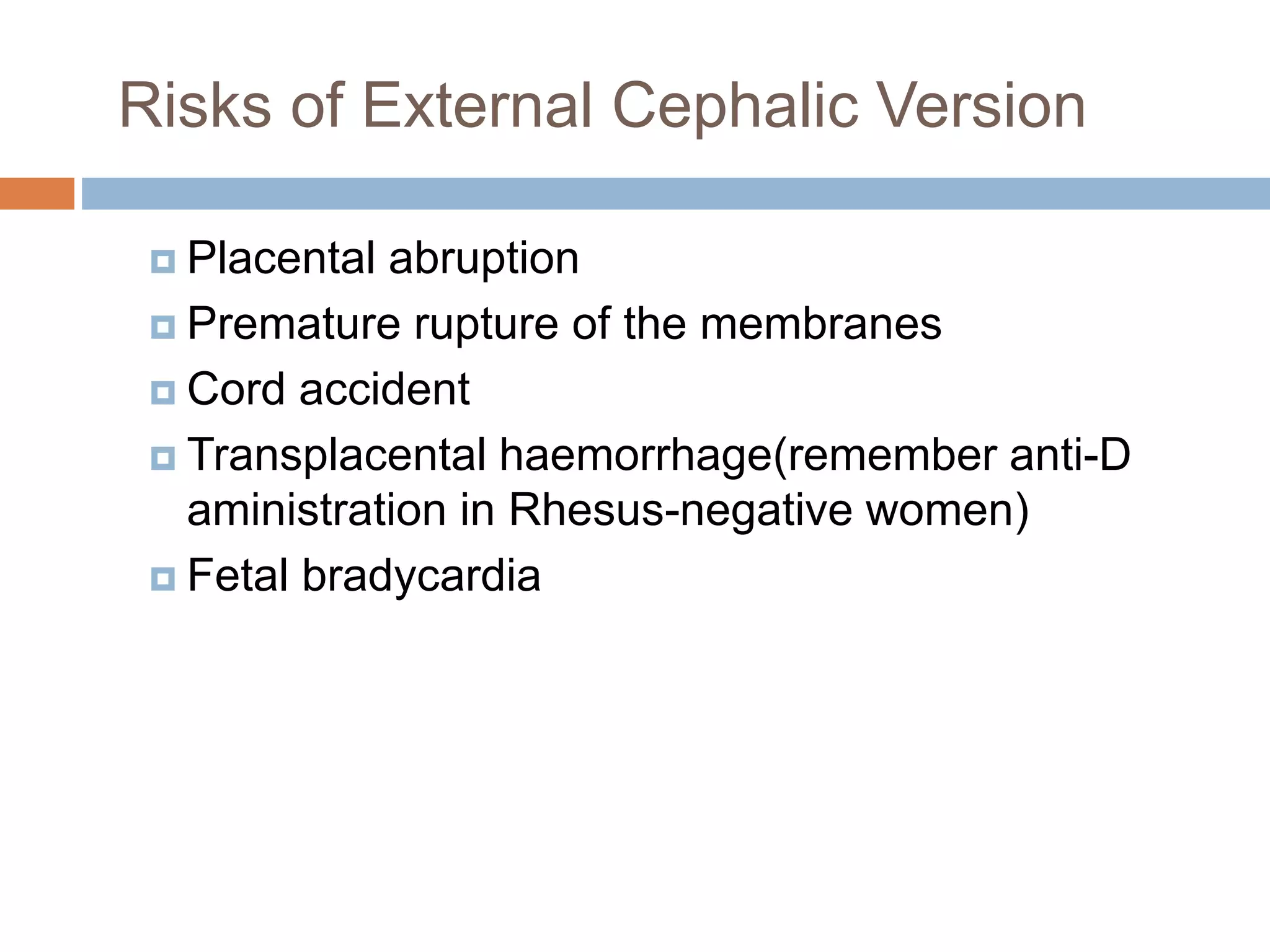
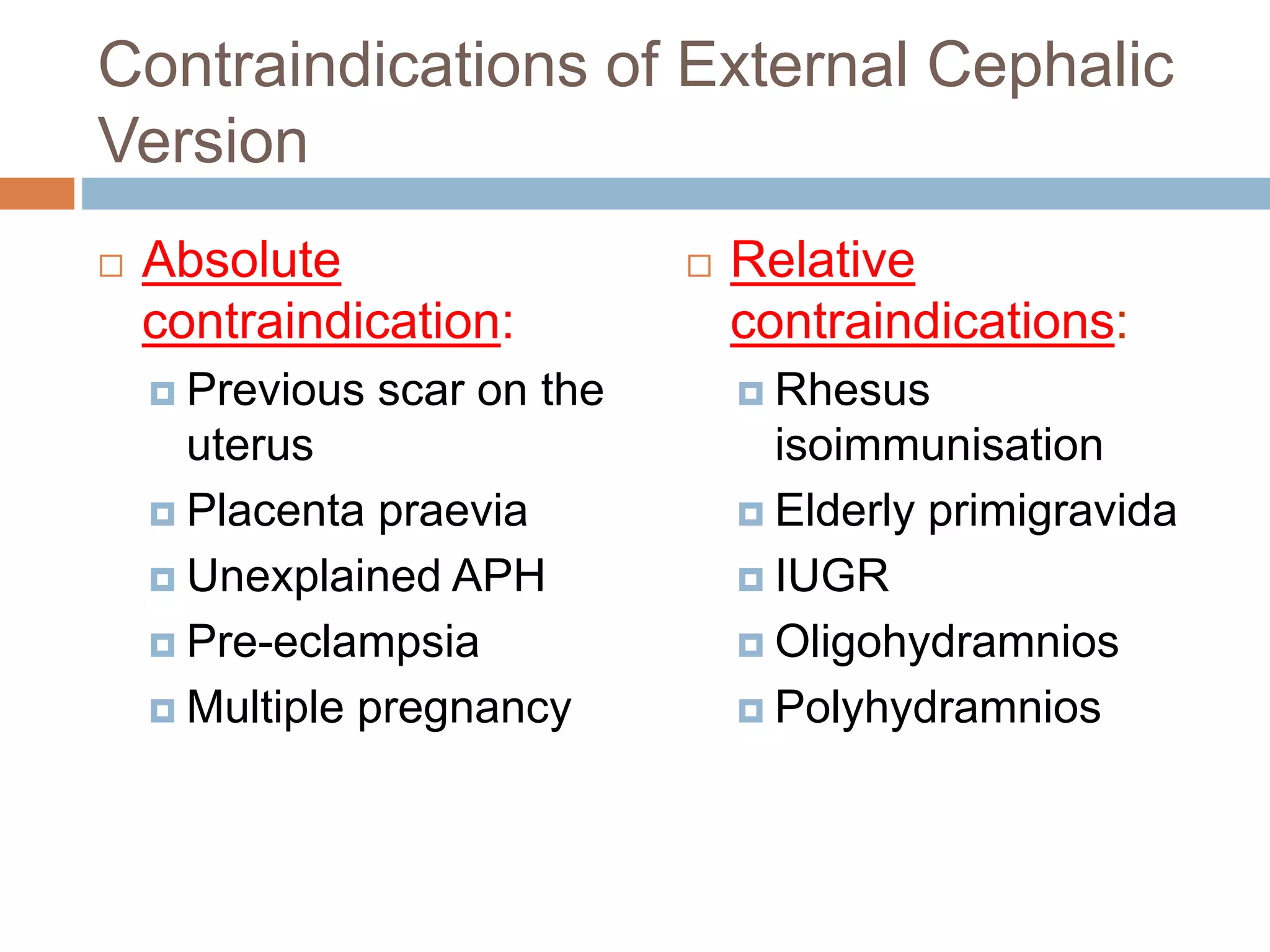
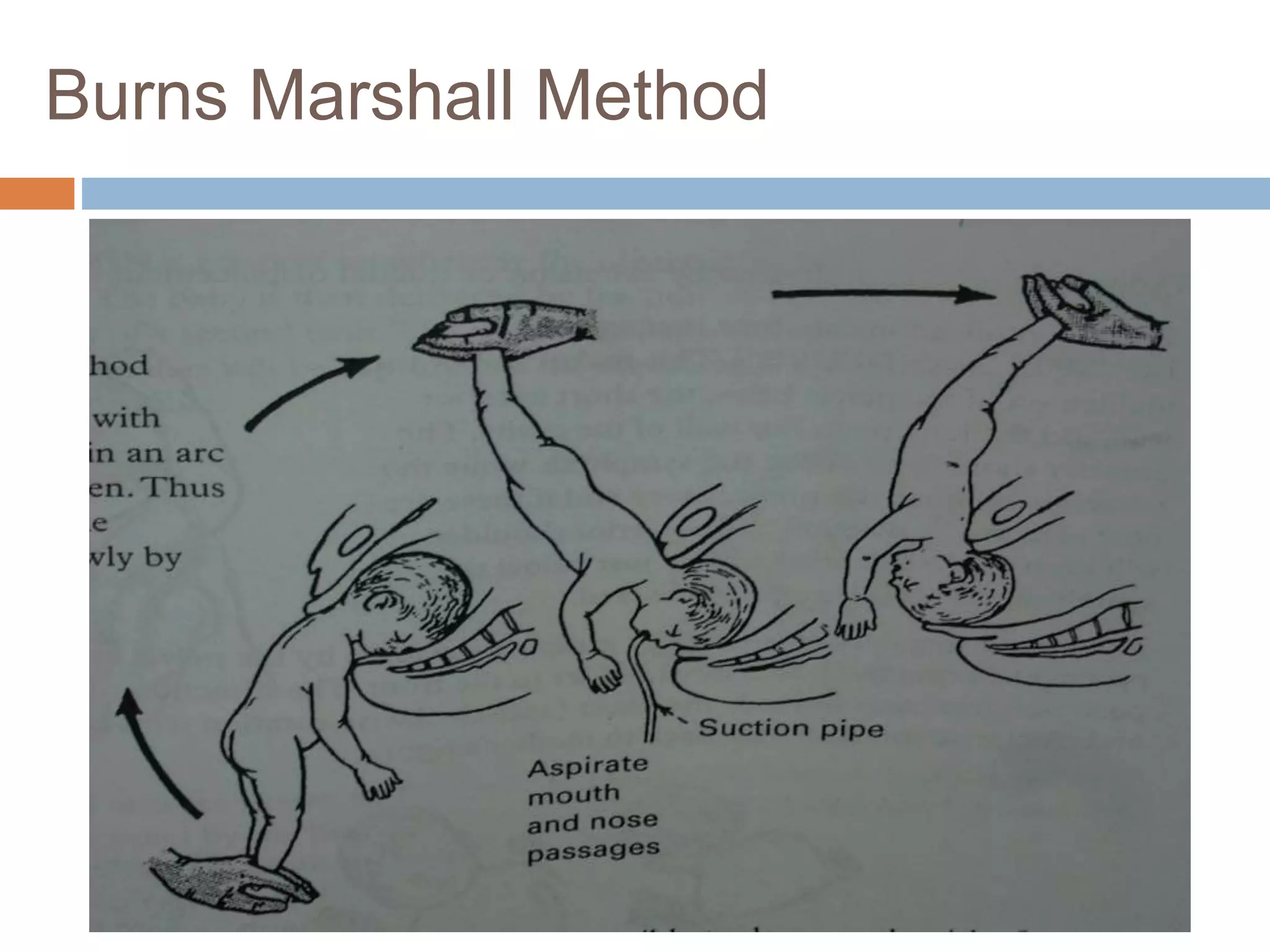
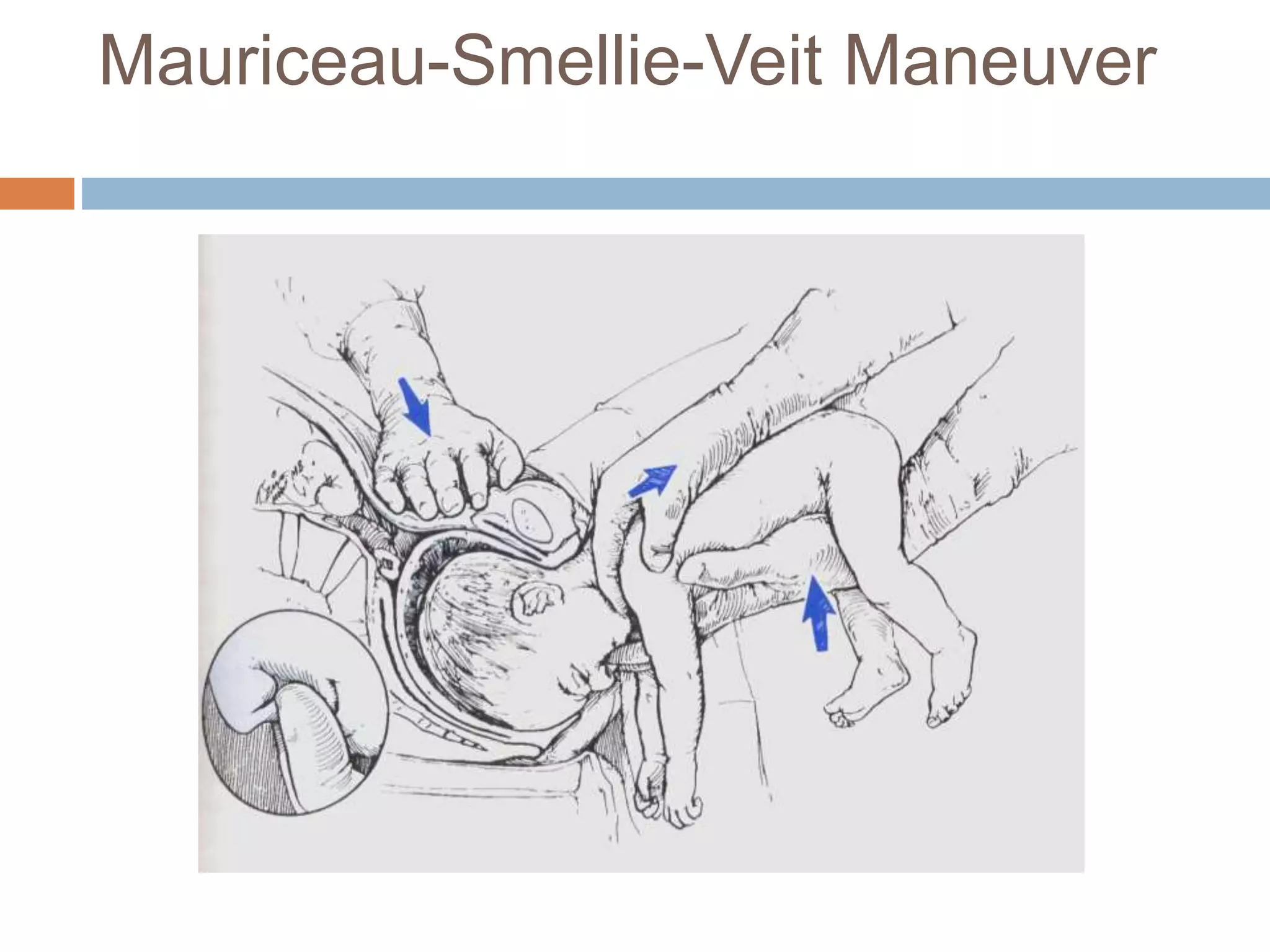
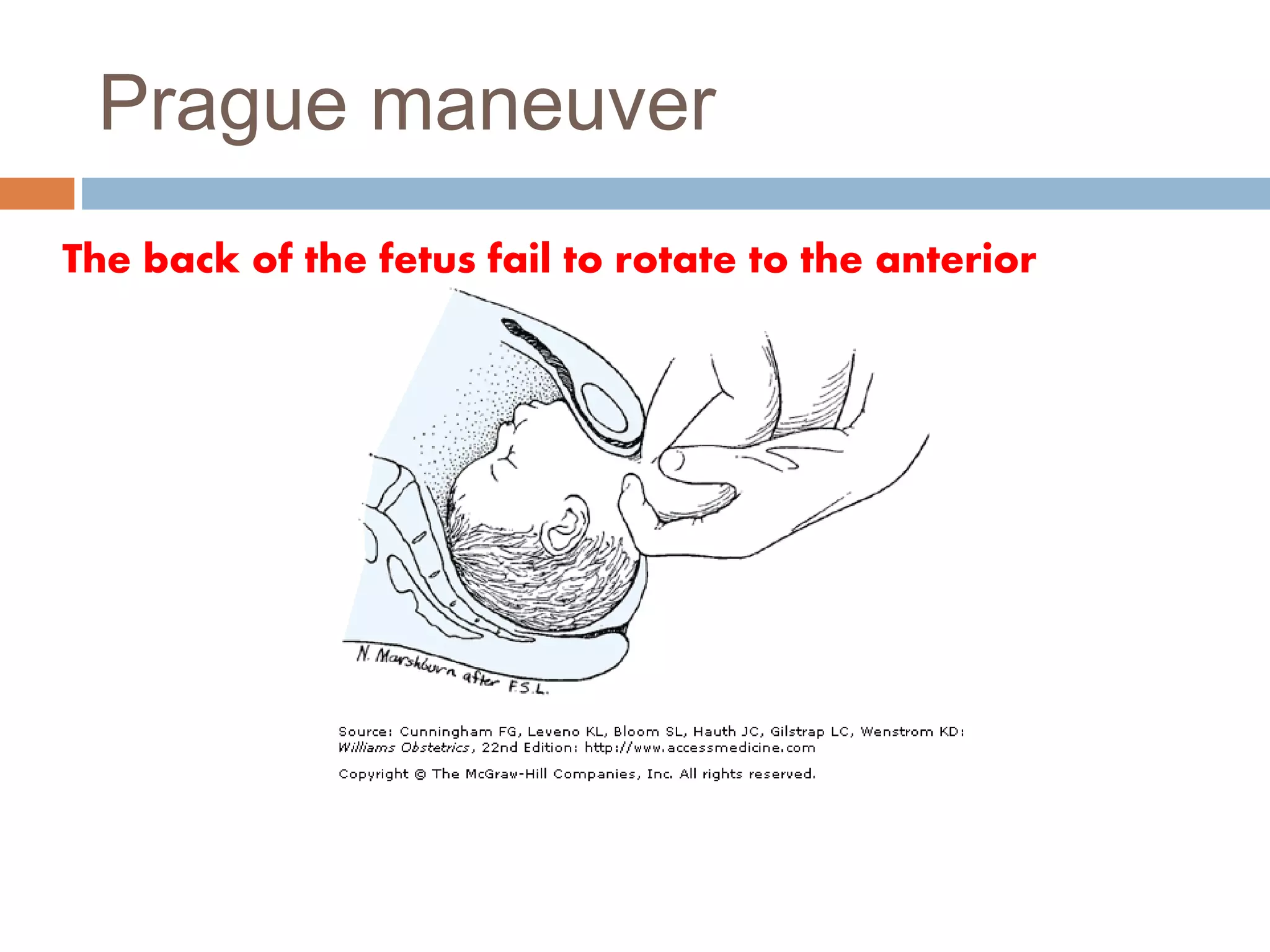
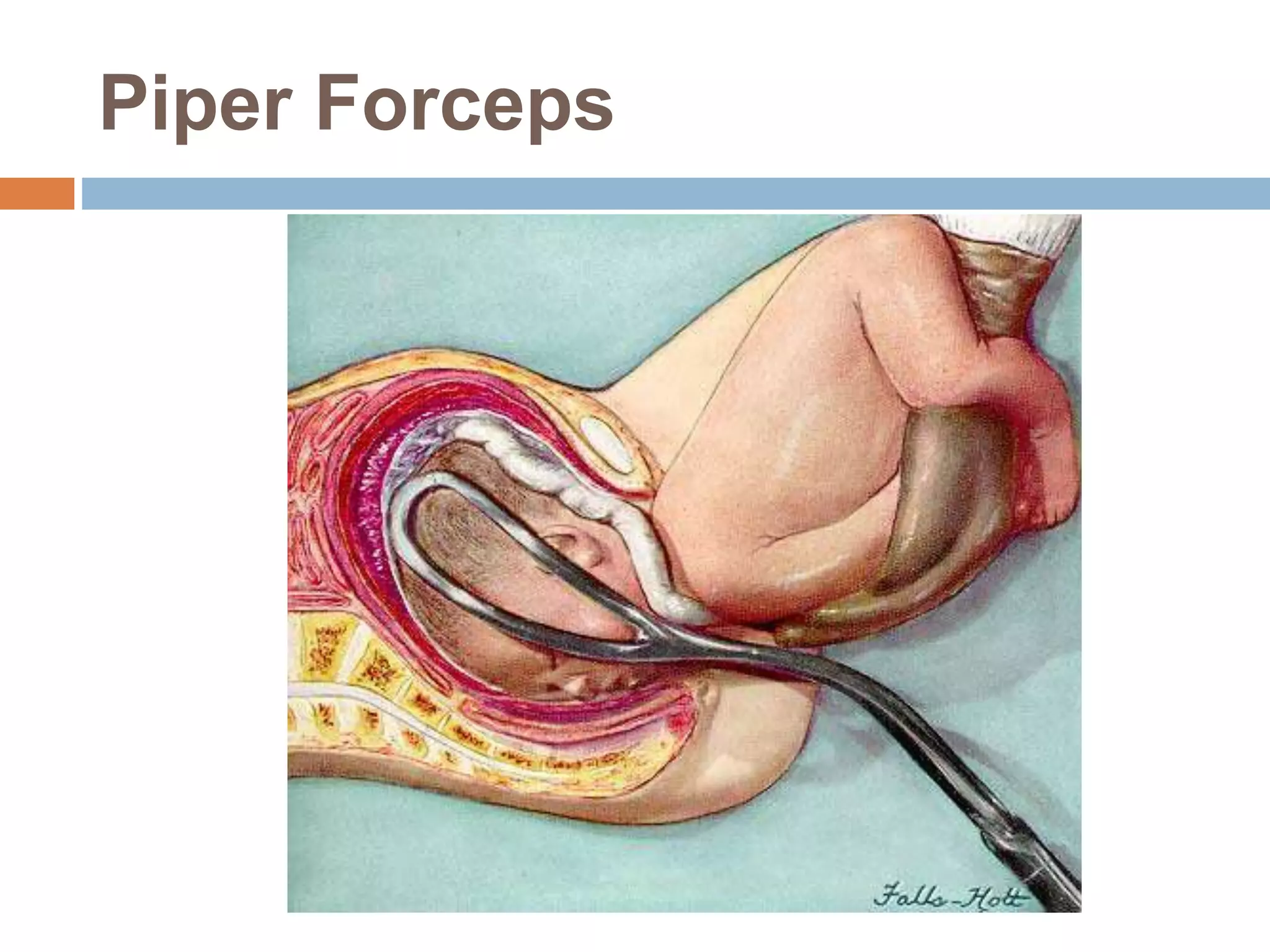

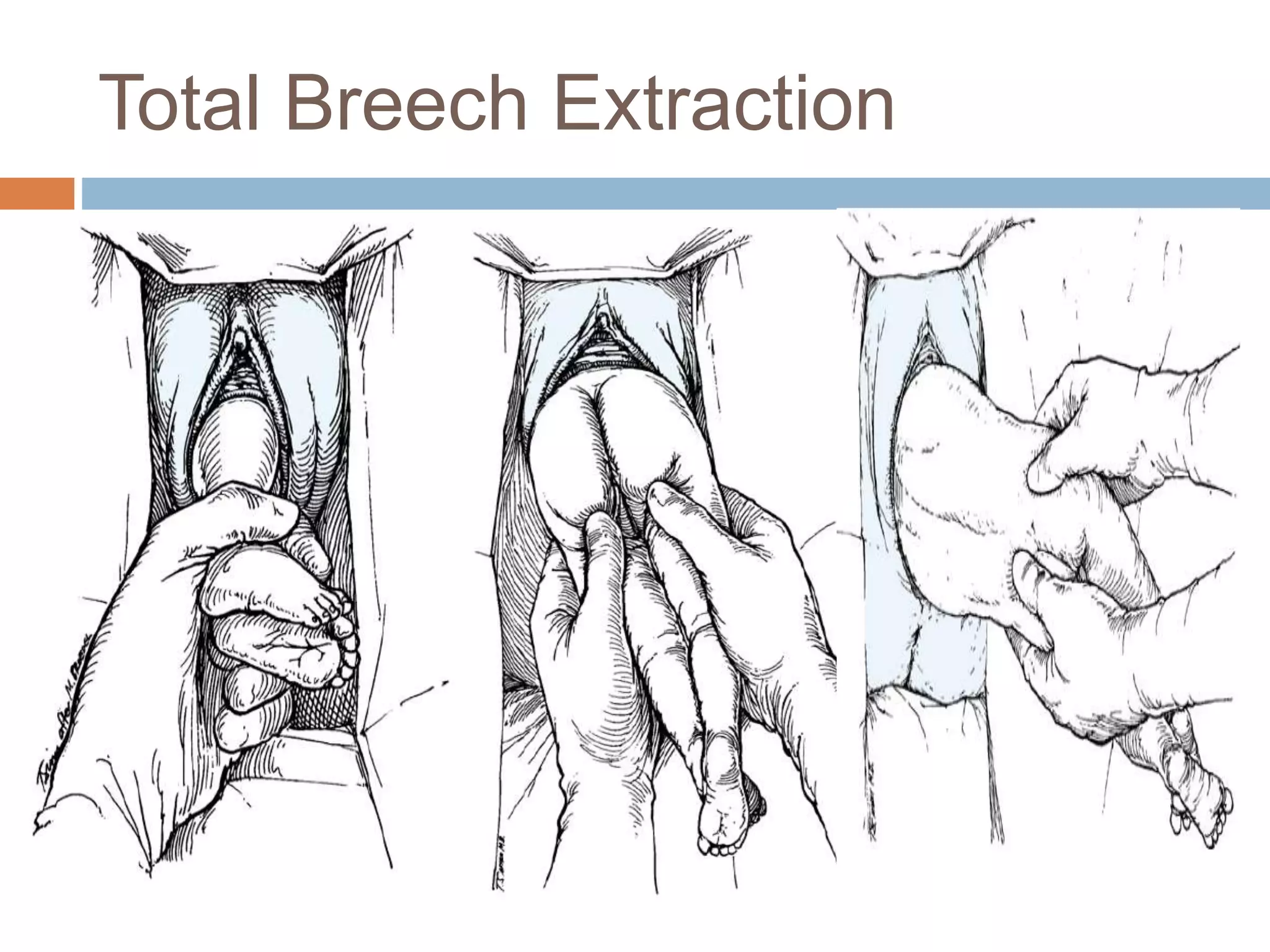


Breech presentation refers to when the fetus is in a longitudinal lie with its buttocks as the lowest part. The document discusses the different types of breech presentations as well as their incidence, classifications, positions, etiology, diagnosis, and management both during pregnancy and delivery. Management during pregnancy includes attempting external cephalic version after 36 weeks to convert the fetus to head-first position. Management during delivery depends on factors such as gestational age and fetal/maternal conditions, and may involve vaginal delivery with assistance, total breech extraction, or cesarean section to avoid risks to the mother and fetus.





























![Breech presentation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/breechpresentationautosaved-211128120250-thumbnail.jpg?width=640&height=640&fit=bounds)