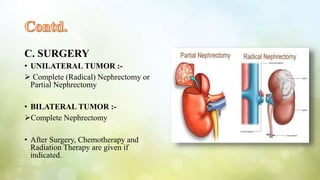
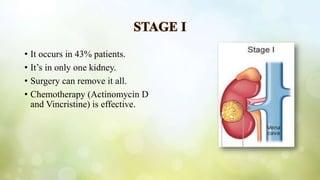
Wilm's tumor, or nephroblastoma, is a malignant kidney cancer primarily affecting children aged 3-5 and usually occurs unilaterally. Diagnosis includes physical examination, imaging tests, and urinalysis, while treatment consists of surgery, chemotherapy, and radiation therapy based on cancer stage. The goal is to cure the child while minimizing side effects, with various treatment protocols depending on whether the tumor is unilateral or bilateral and its extent of spread.


















































![Wilm's tumour - The most common kidney tumor in children - Dr Vishnu A [VCR],...](https://cdn.slidesharecdn.com/ss_thumbnails/vishnu-wilmstumour-210312145616-thumbnail.jpg?width=640&height=640&fit=bounds)












![metabolic disorder in pegnancy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/metabolicdisorderinpegnancyautosaved-240725113357-734a2382-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















