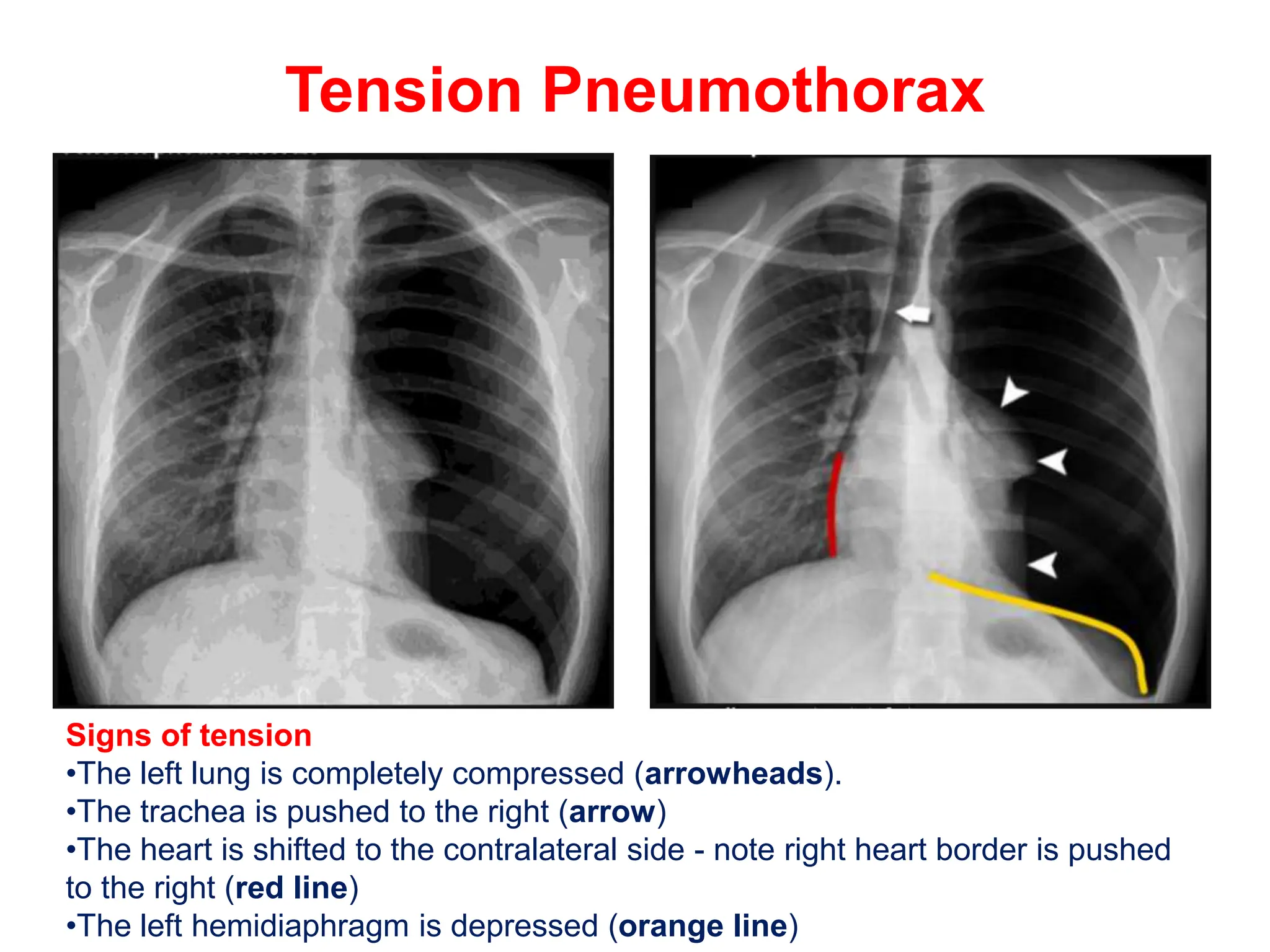
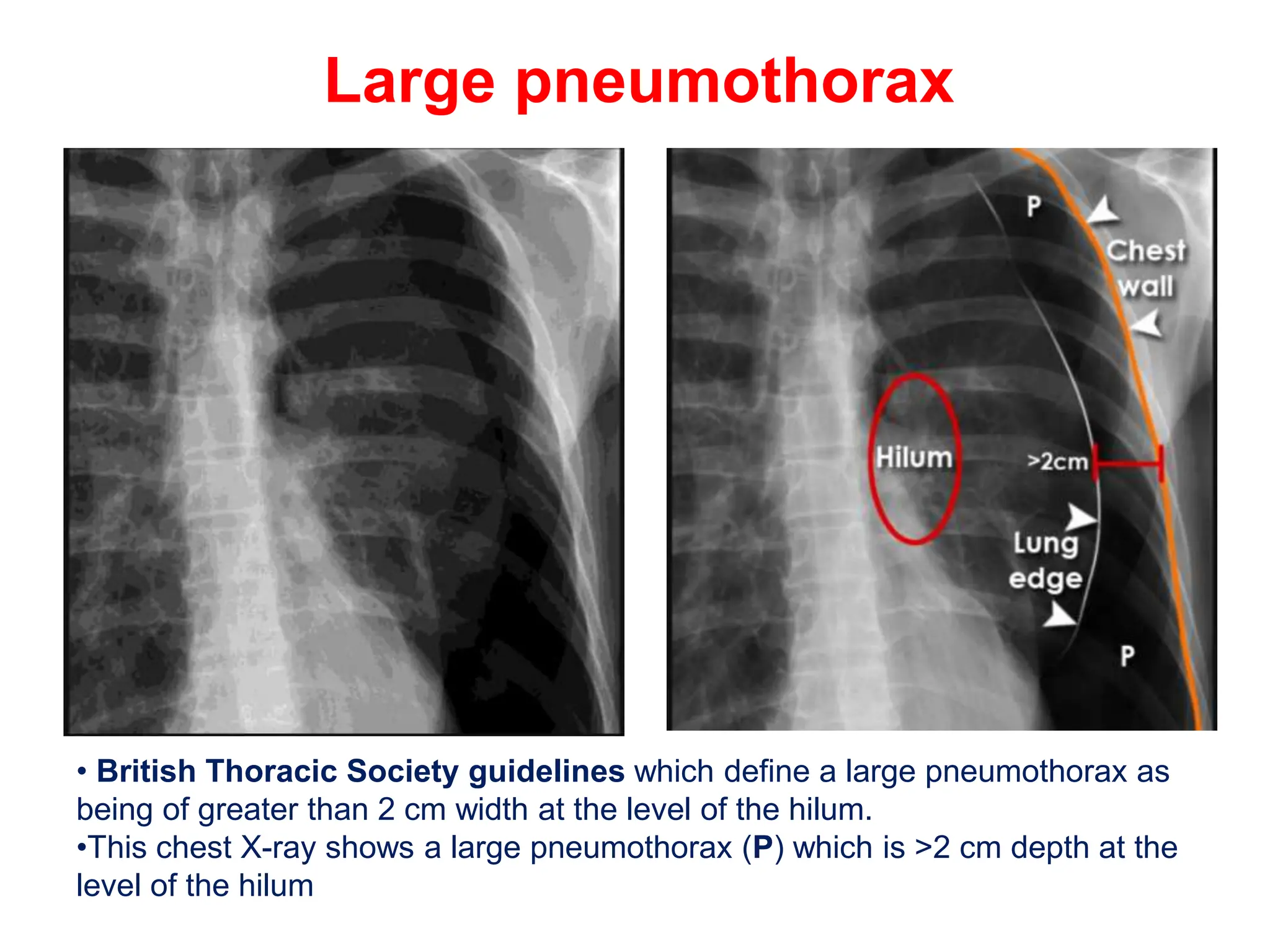
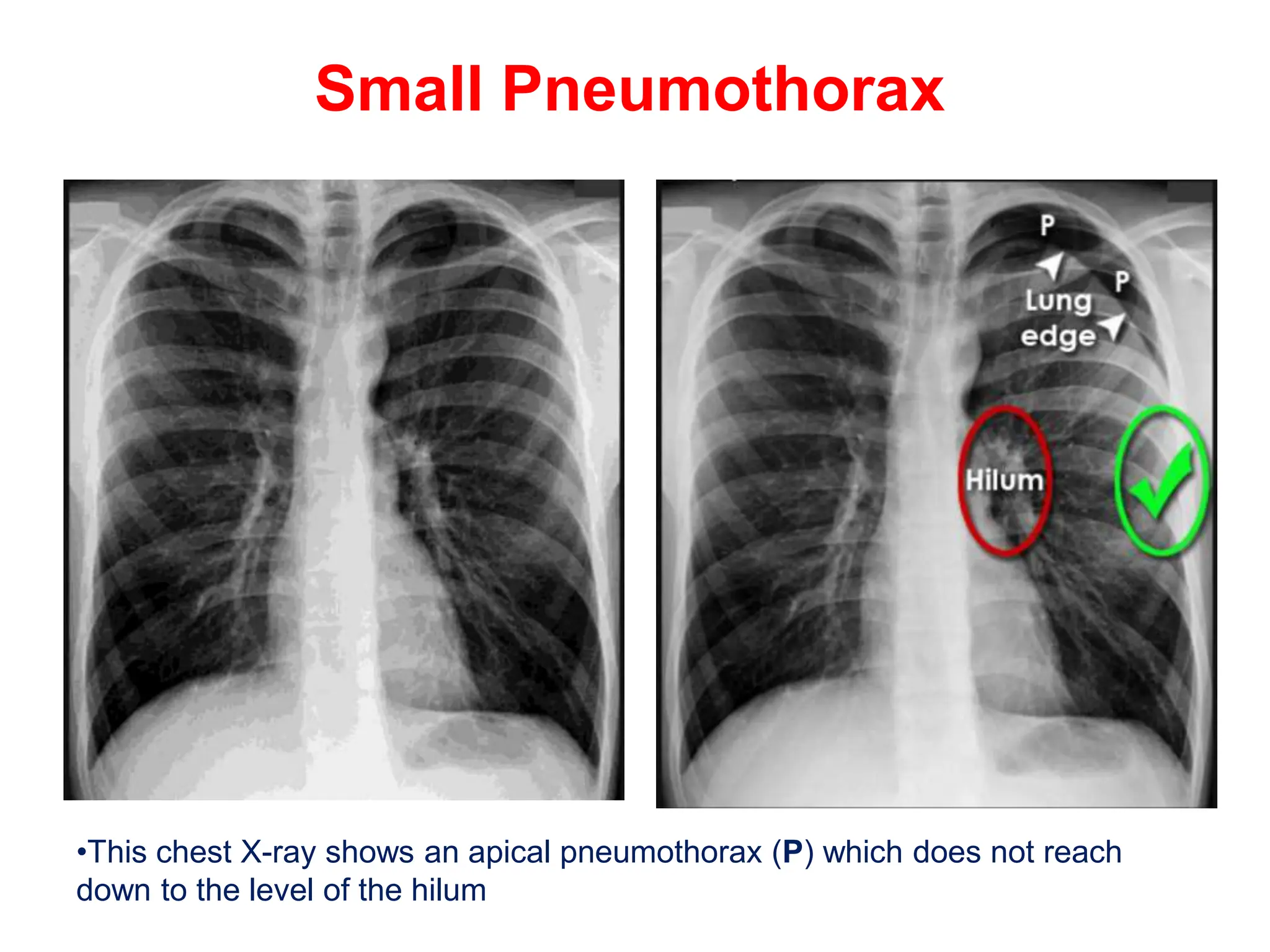
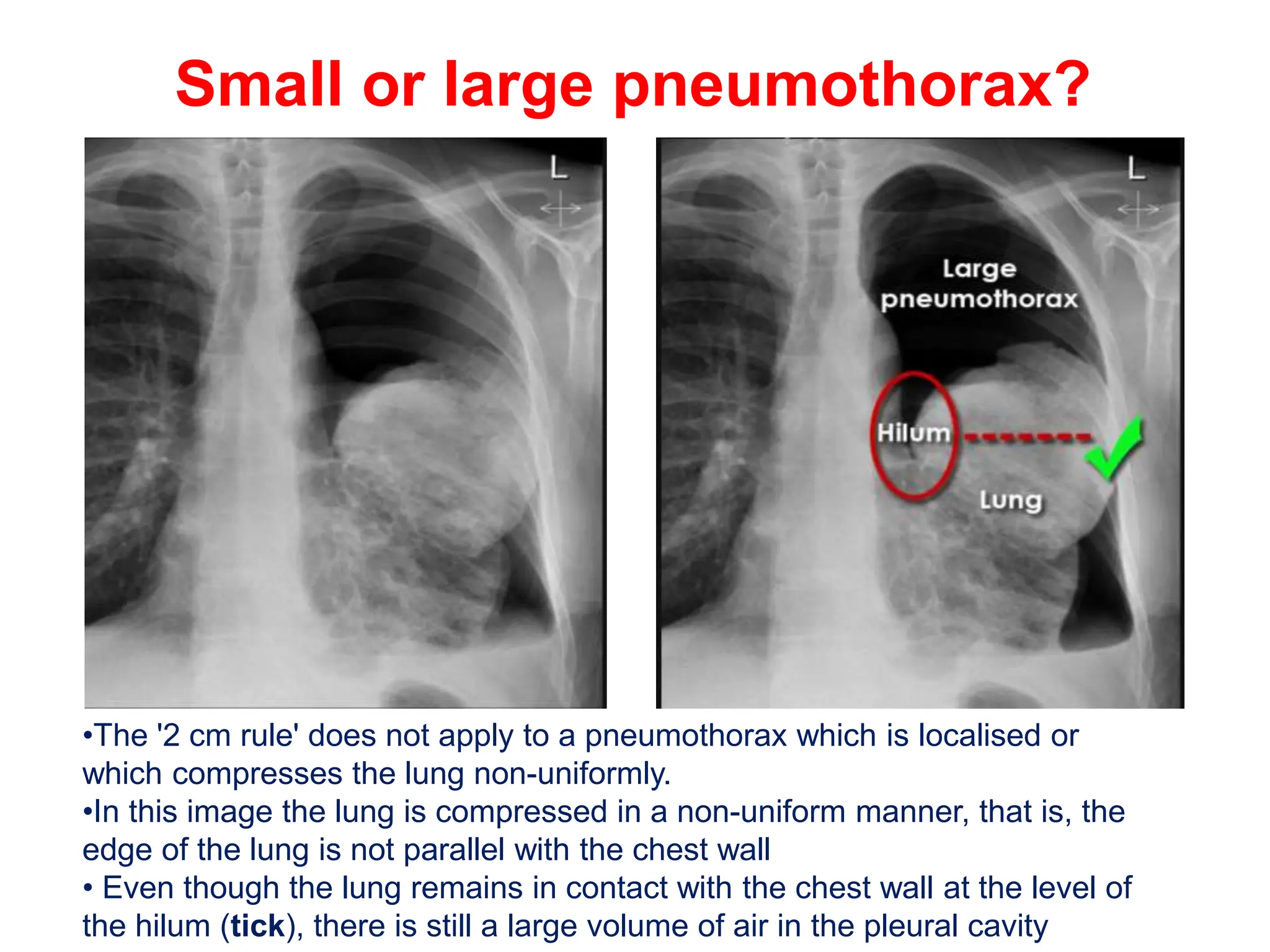
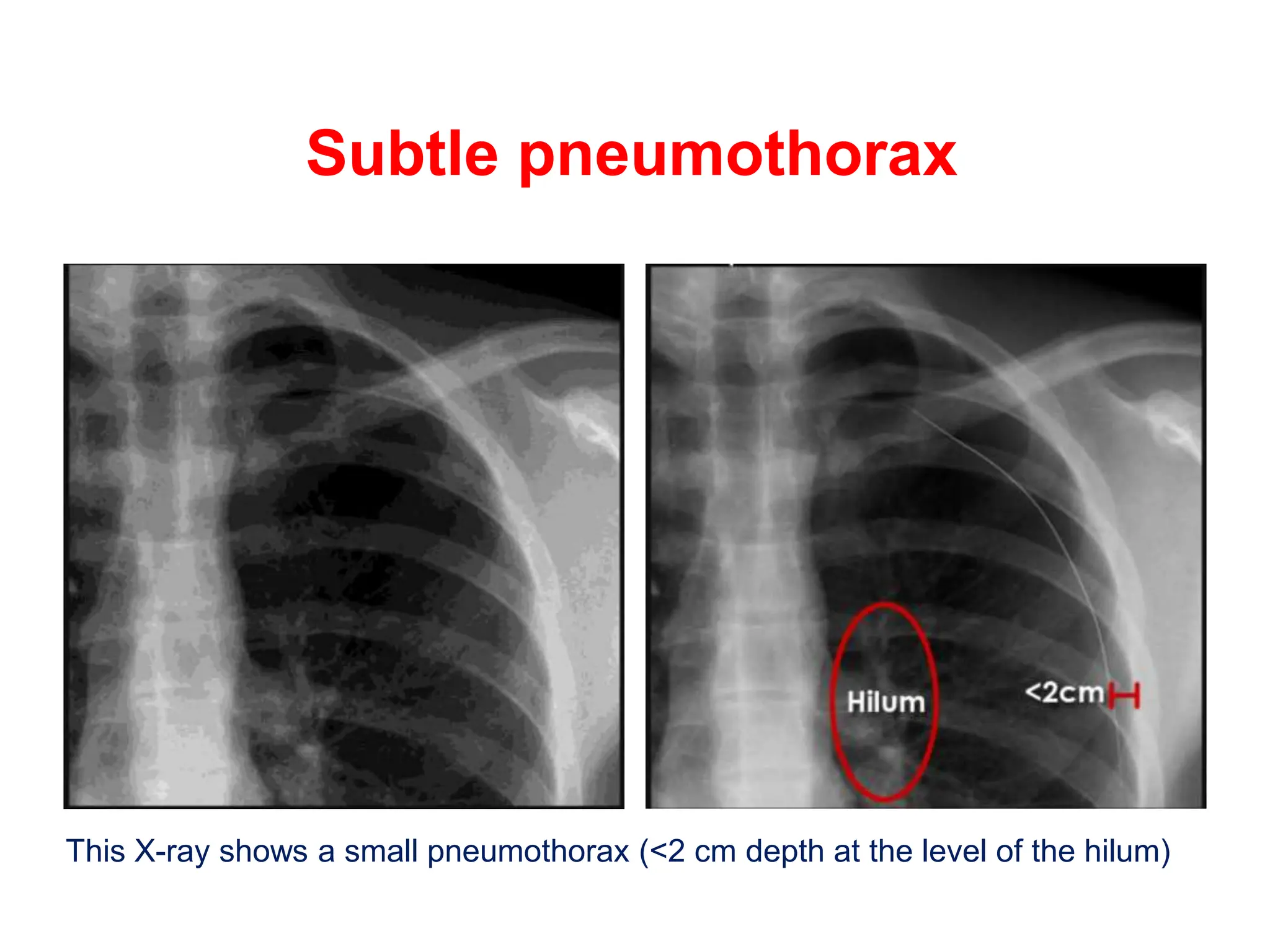
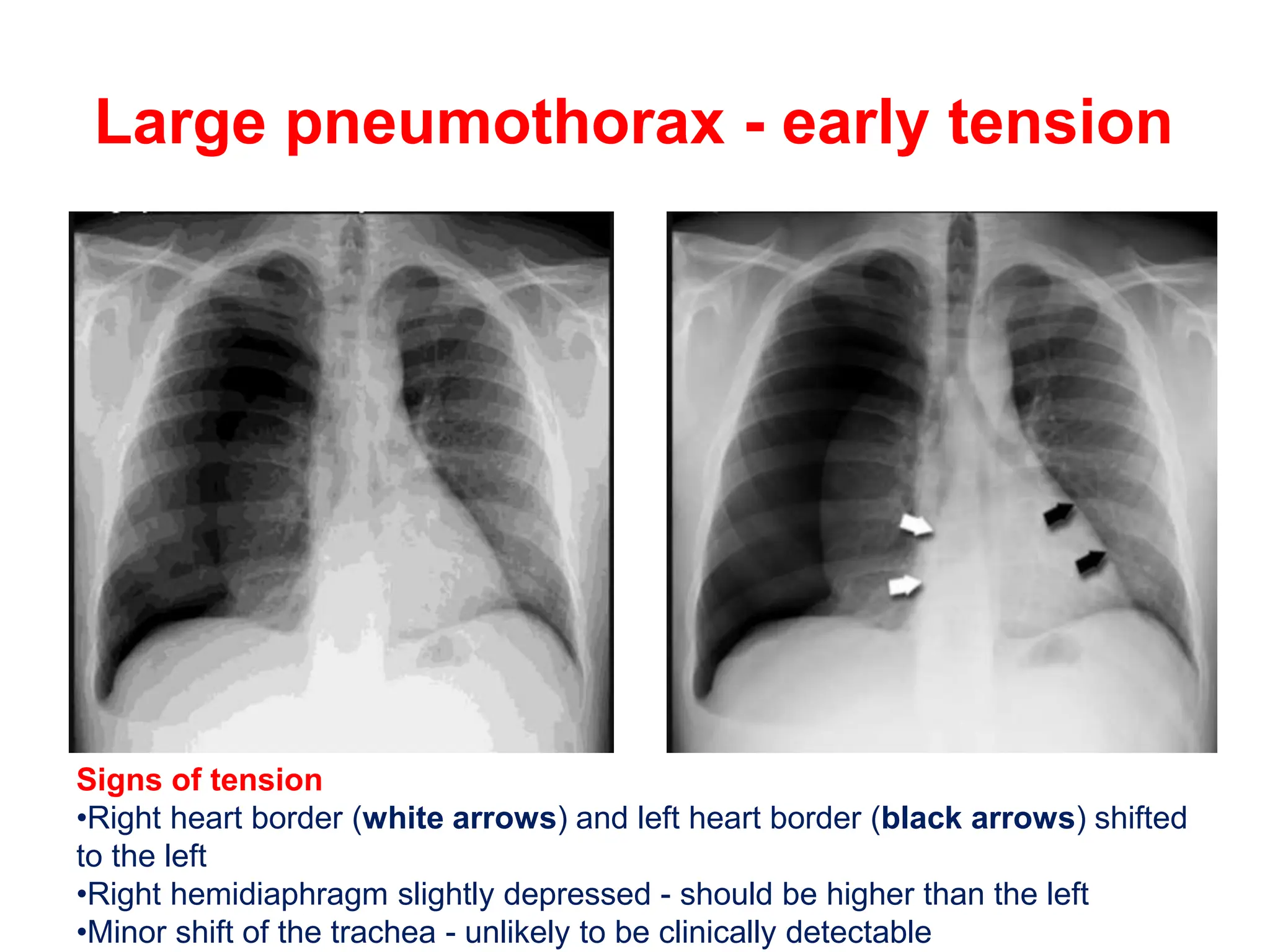
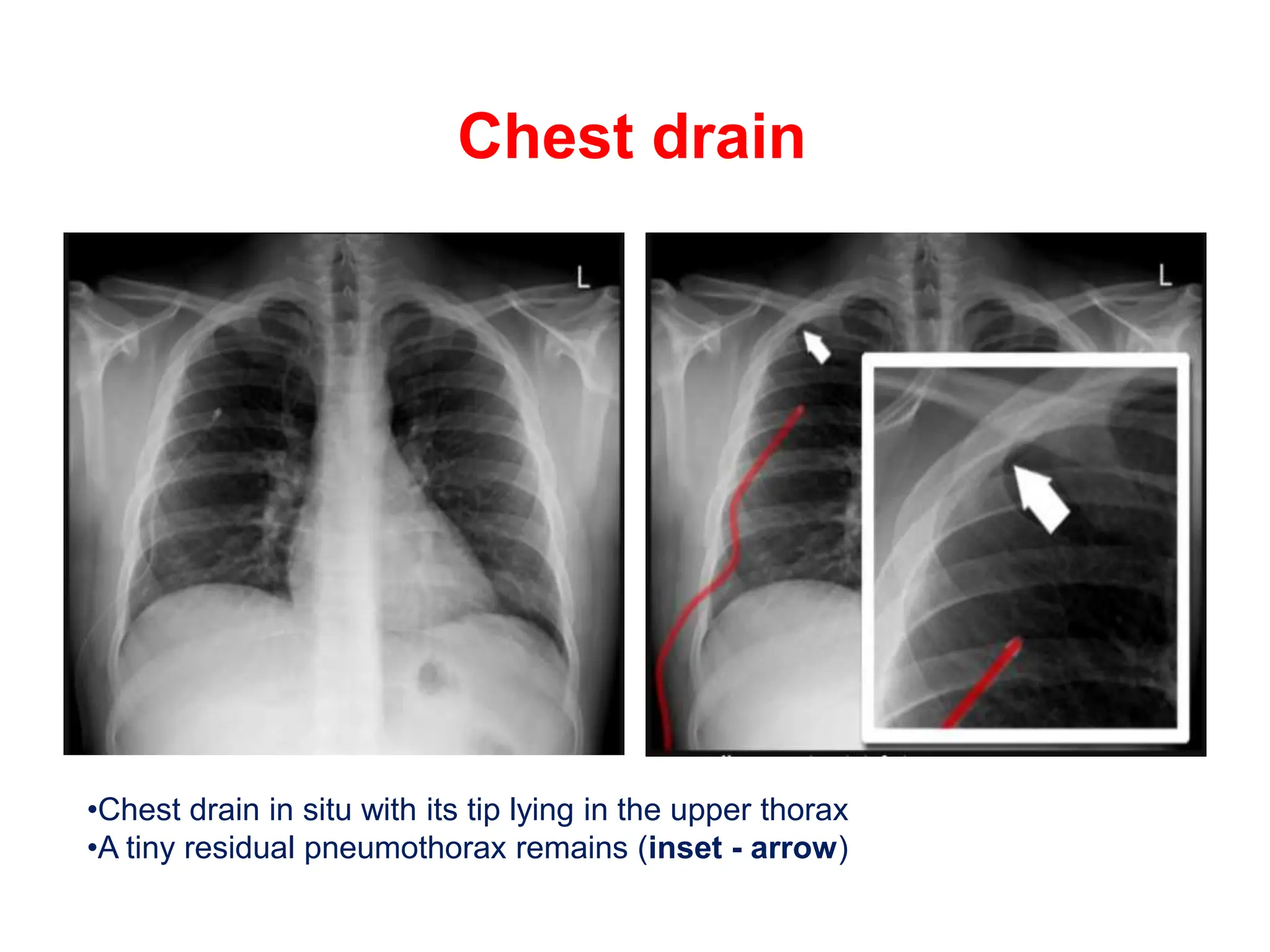
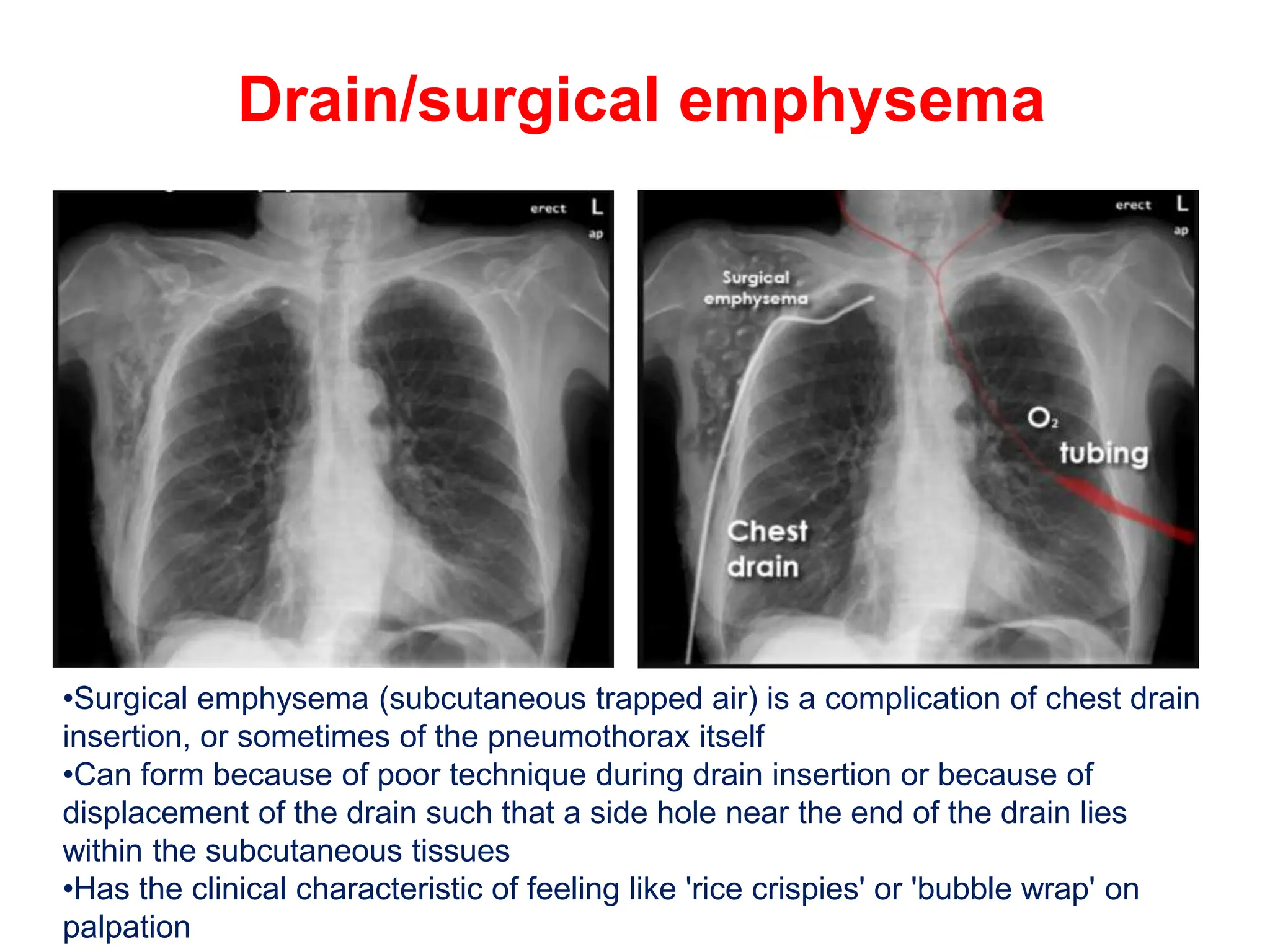
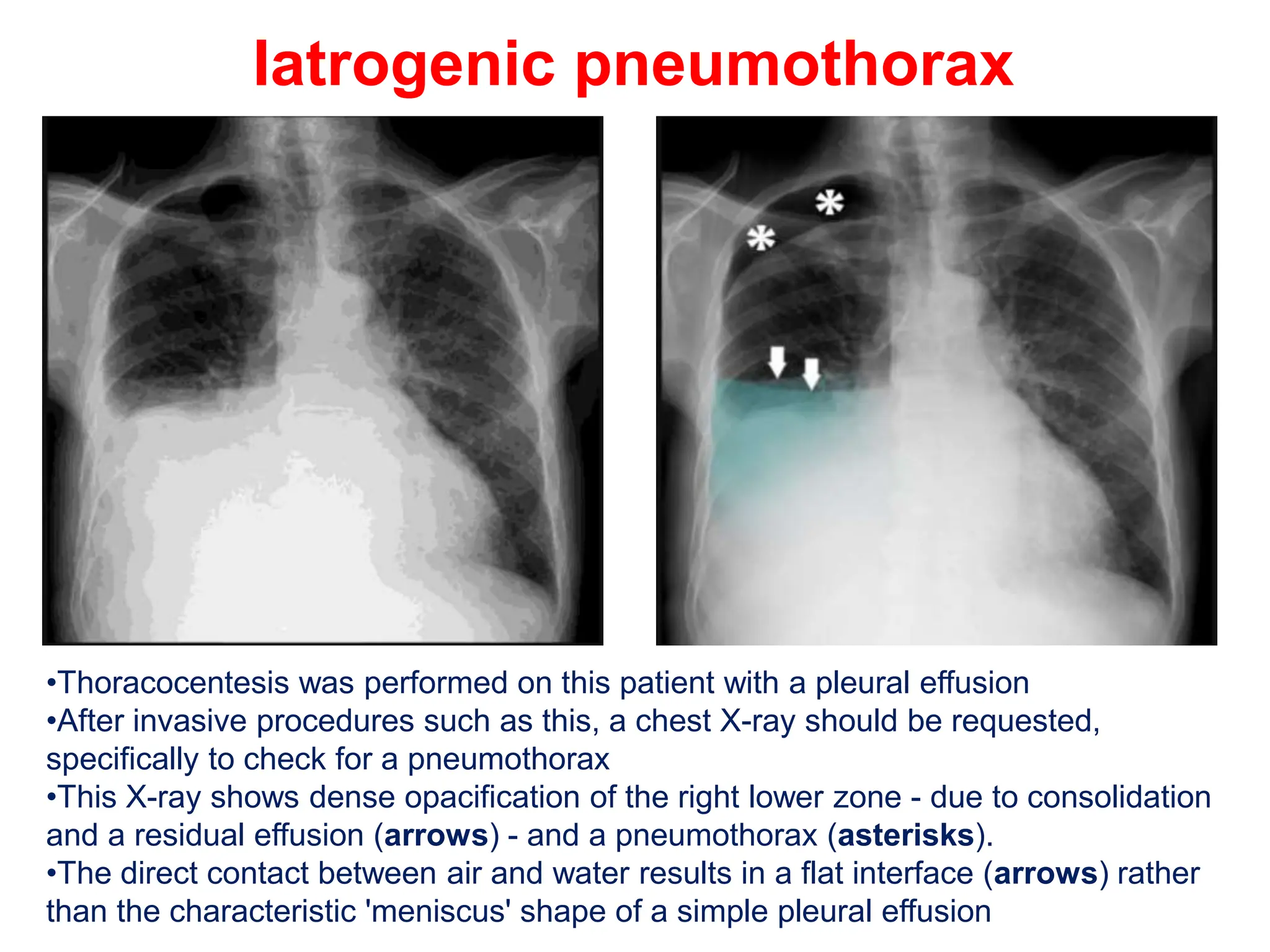
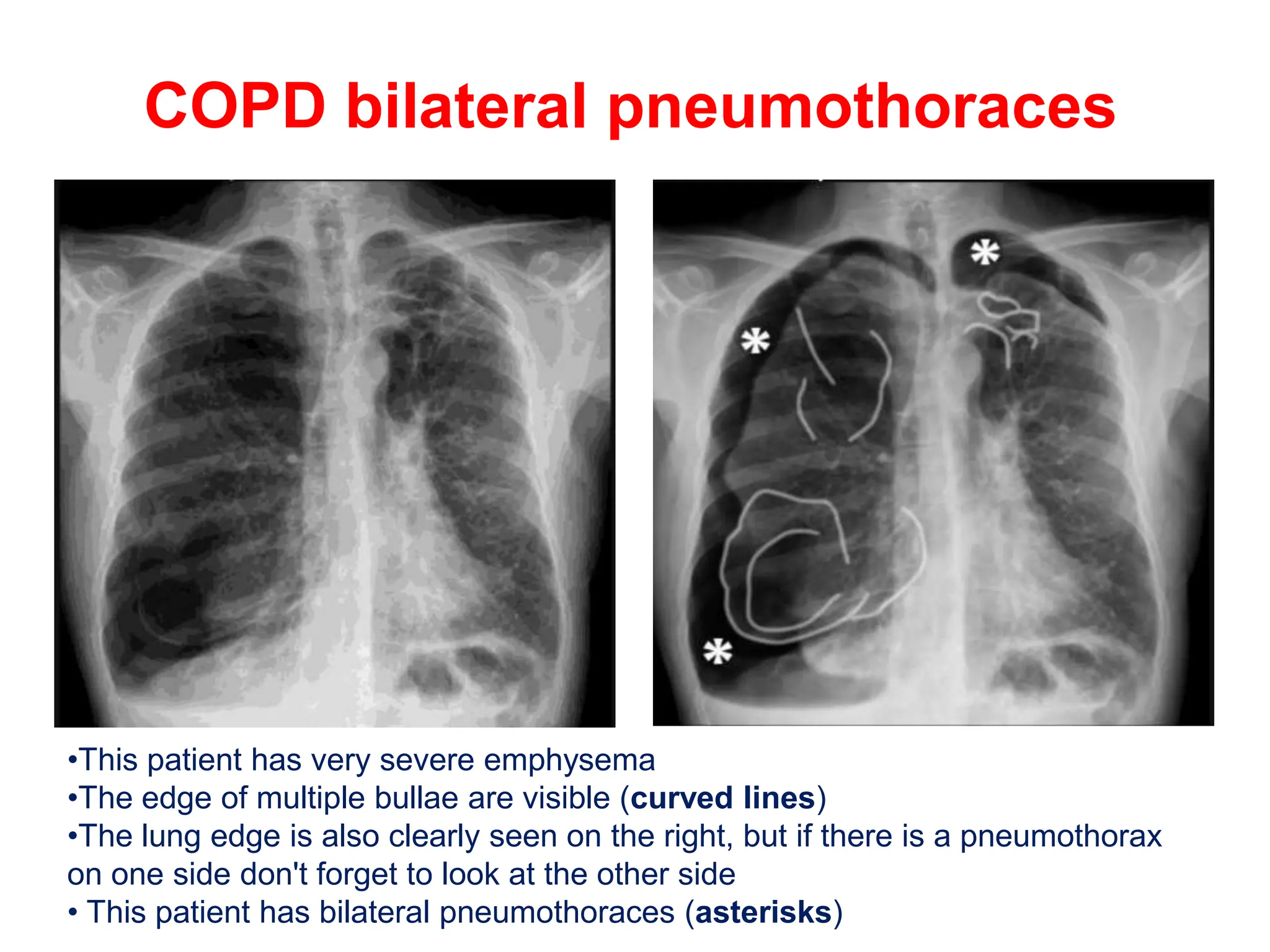
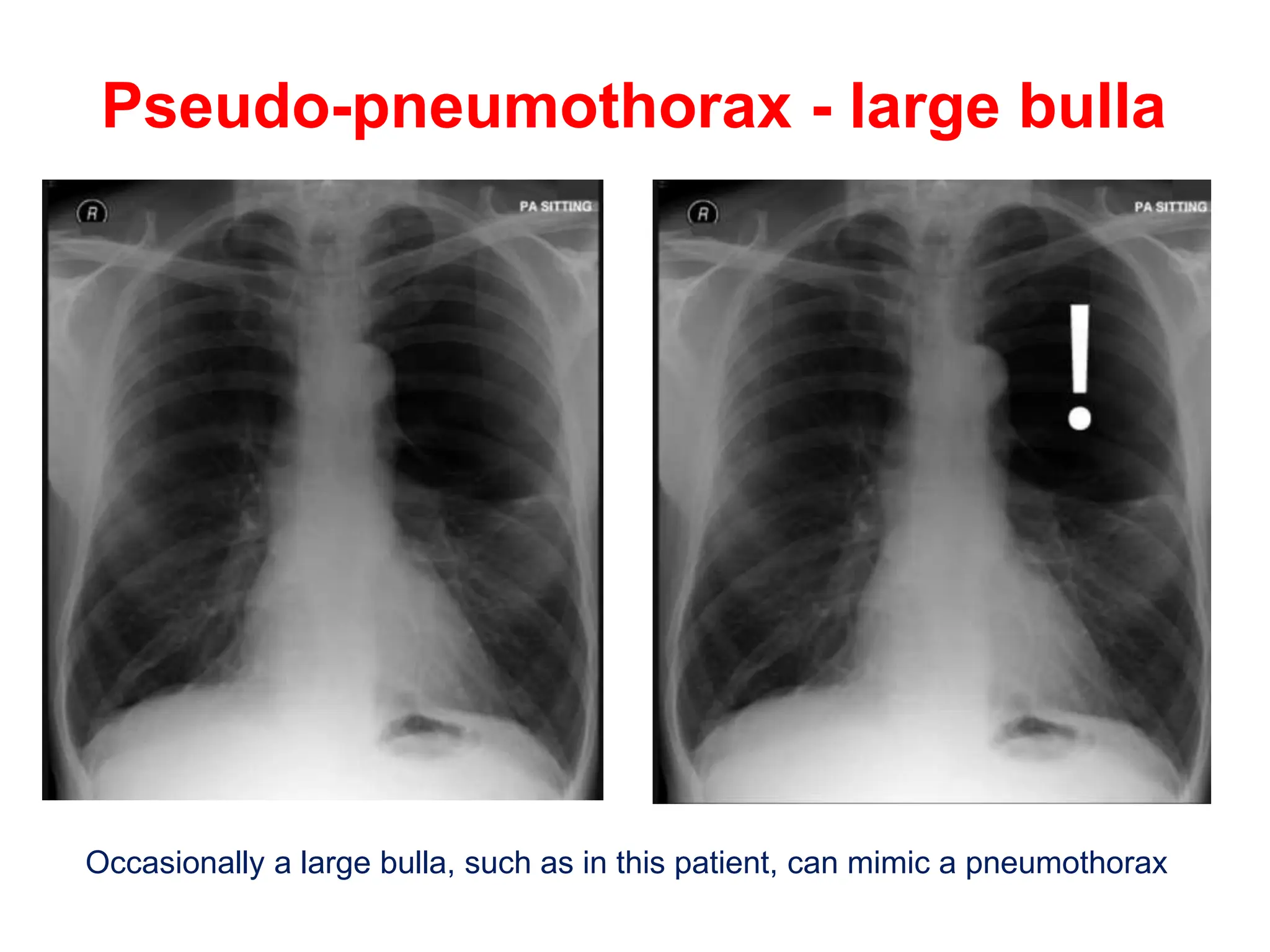
The document discusses various findings related to pneumothorax as shown in X-rays, including hyperlucency, absent lung markings, and visualization of the collapsed lung margin. It outlines the distinctions between small and large pneumothoraces based on chest X-ray measurements, as well as signs of tension pneumothorax. Additionally, it covers complications from procedures like thoracocentesis and highlights conditions such as bilateral pneumothoraces and pseudo-pneumothorax.