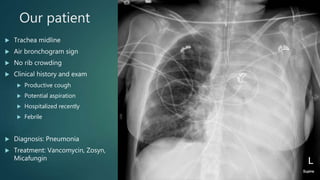
A 28-year-old female with diabetes, chronic pancreatitis, and substance abuse presented with cough, chills, and nausea for 3 days. Imaging showed complete white-out of the left lung with an air bronchogram sign. The differential diagnosis for hemithorax white-out included pulmonary edema, consolidation, or a chest wall/pleural mass. Given the trachea was midline and presence of an air bronchogram sign, consolidation from pneumonia was suspected. The patient was treated with antibiotics.





































![Imaging in opaqe hemithorax [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/imaginginopaqehemithoraxautosaved-161030071708-thumbnail.jpg?width=640&height=640&fit=bounds)
























































