Download as PDF, PPTX
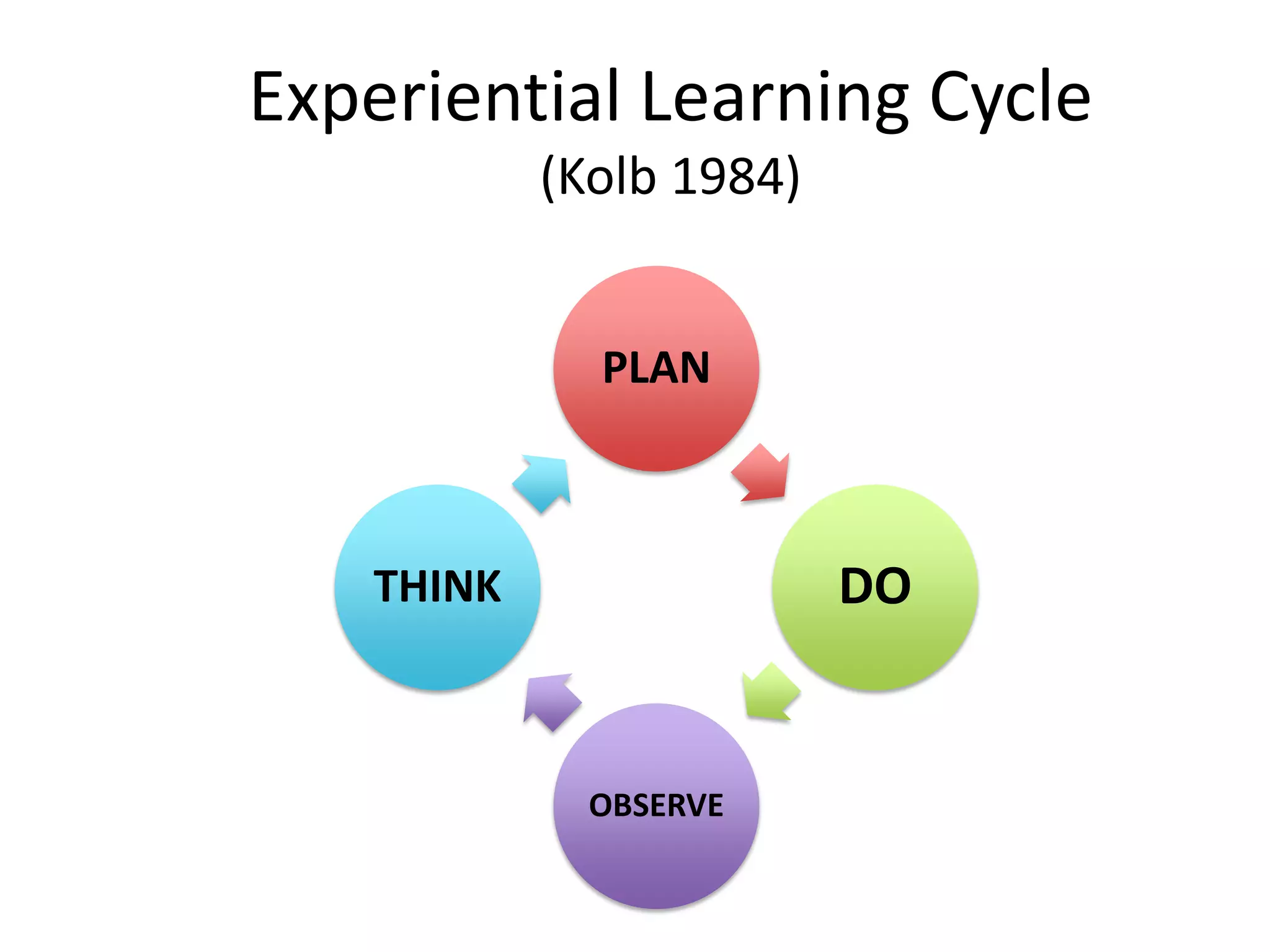

The document outlines key learning objectives for effective clinical teaching, emphasizing the importance of planning and understanding various learning theories. It highlights the experiences of both doctors as teachers and students as learners, presenting effective techniques and methods for conducting successful teaching sessions. Additionally, it discusses the experiential learning cycle and offers practical guidelines for preparing teaching materials and engaging students.